To members of the Alabama Legislature,
Alabama is struggling. Even after Governor Ivey issued an emergency stay-at-home order, the average number of new coronavirus cases continues to rise. And despite those climbing case numbers, Alabama is moving forward with reopening its economy. To accomplish a successful recovery, residents must have confidence that it is safe to be in public and workers must be able to work in safe environments without fear for their health or the health and safety of their families. We are asking that you support the following recommendations so that Alabama will use the $1.9 billion under the Coronavirus Relief Fund to heal and protect the communities who have and will continue to shoulder the high costs of this crisis.
The Alabama Legislature, in consultation with Governor Ivey, has divided these federal funds into large categories of spending. Governor Ivey now has provided a method by which you and your colleagues may request release of the funds for coronavirus-related expenditures.
We recognize that $1.9 billion is inadequate to address the long-term needs of Alabamians as the present economic crisis continues to unfold. Consequently, you and your colleagues will need to find additional revenue sources to ensure that Alabama’s economy does not weaken further and that its residents are sufficiently protected from future spikes in infections. We look forward to working with you on those longer discussions.
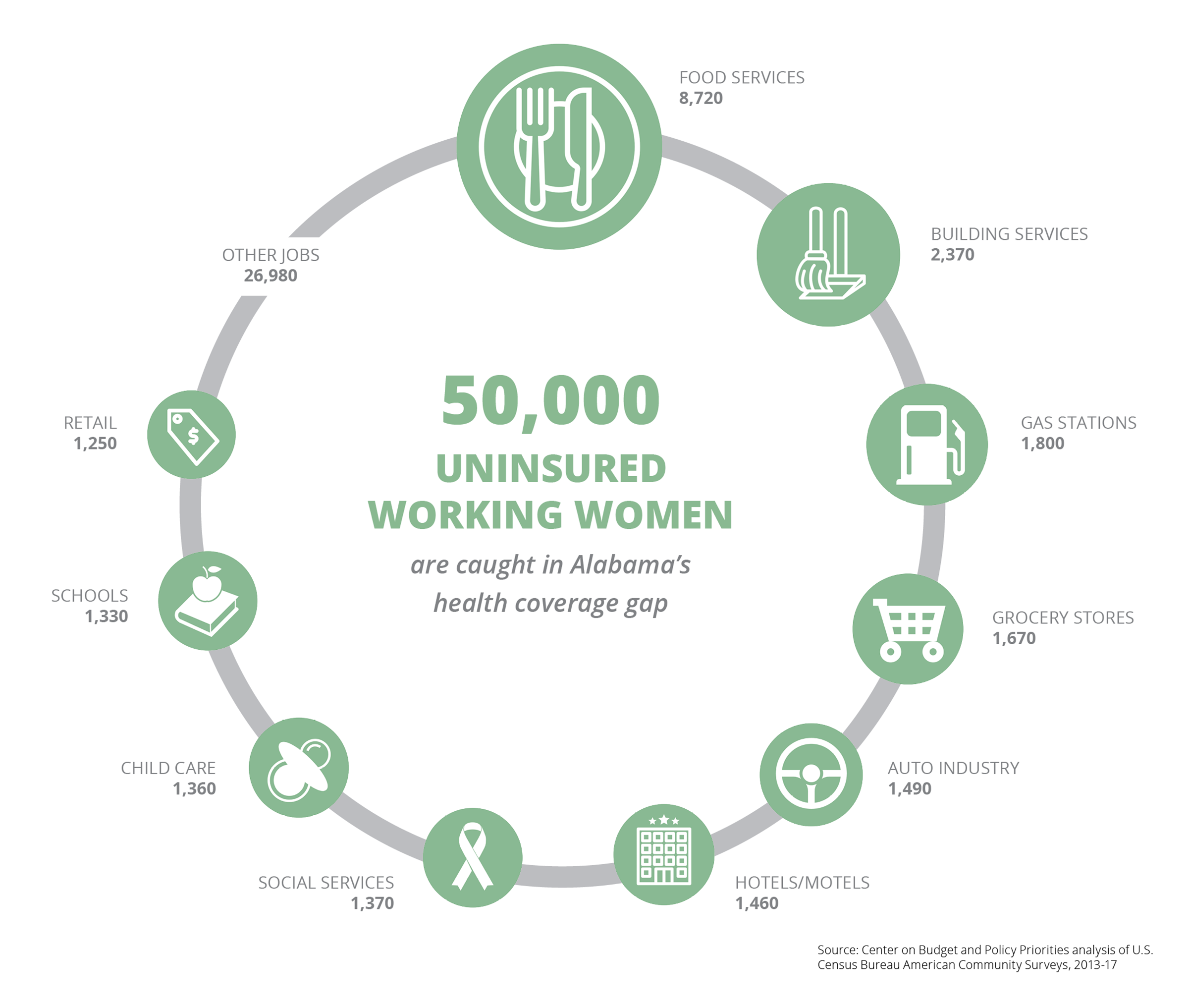
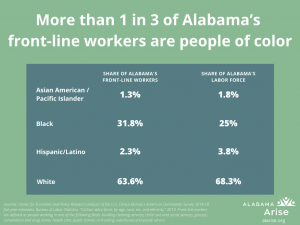
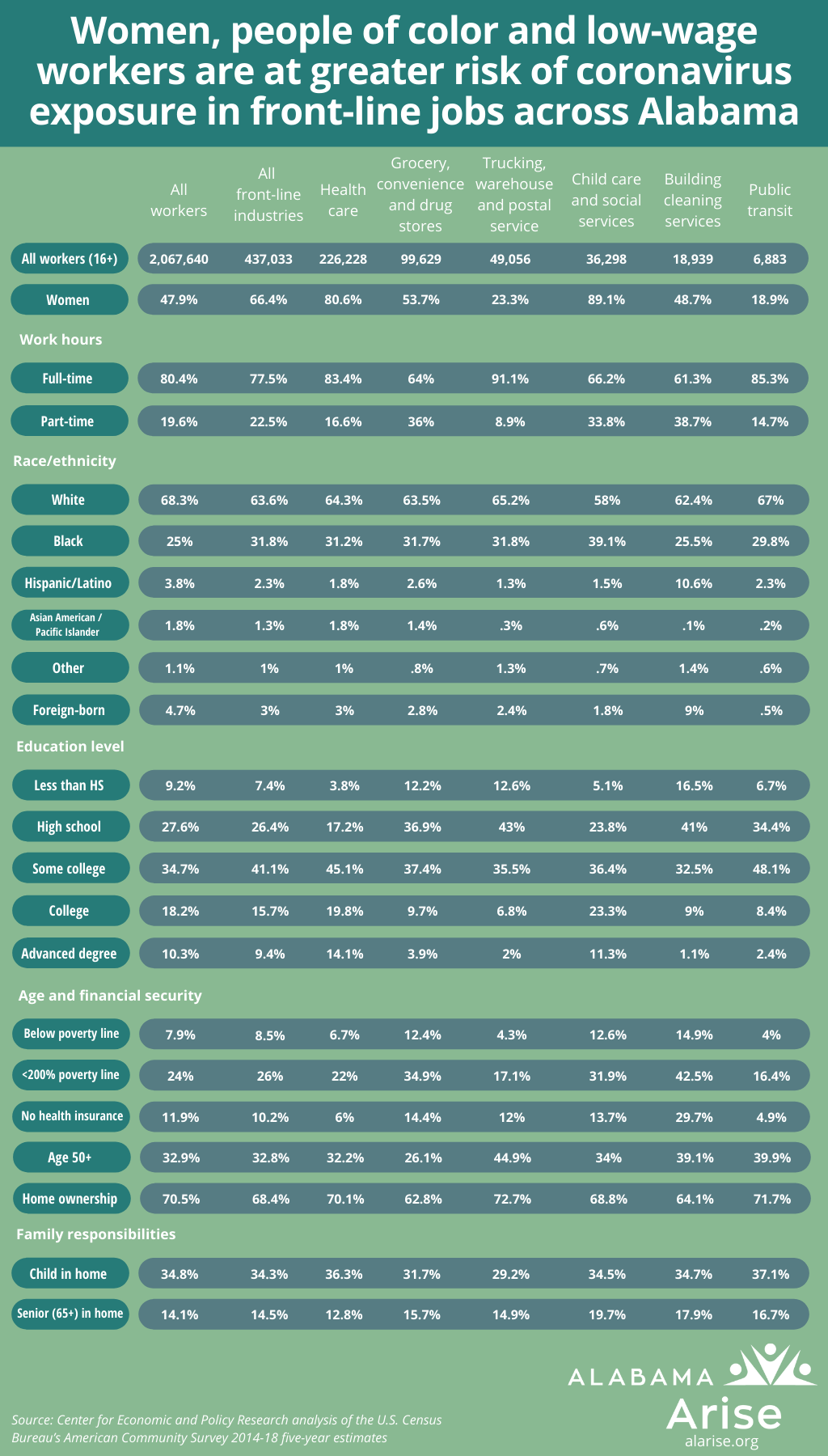
Our recommendations aim to provide support where it is most needed, reflecting the disparate impact of the crisis. Highly educated workers have largely been able to work from home. Low-wage and many essential workers have not. Unemployment rates are highest for workers who have less than a bachelor’s degree and are higher in our Latinx and Black communities. We have also seen the largest gender gap in unemployment, where women experience unemployment at a nearly 3% higher rate than men. Our response to the pandemic and our use of the Coronavirus Relief Funds need to heal this harm, not exacerbate the disparities that already exist.
However the taxpayer-funded payments are distributed, they must be openly accounted with reasonable but sufficient detail. In addition to public reporting of expenditures, the Department of Examiners of Public Accounts must be authorized to audit receipts and expenditures of all agencies within its purview and to request accounting from other CARES Act funding recipients.
Ensuring safe workplaces and families
As Florida and Georgia have shown, merely reopening the economy does not bring back customers or jobs. Both states have seen ongoing unemployment claims at rates higher than other states in the nation. Alabama must ensure that workplaces are safe, that workers’ families are cared for, and that state and local services are ready for people to come back before the more than 500,000 newly unemployed can return to work. These recommendations focus mostly on needs that can be met with the $300 million earmarked for supporting businesses, nonprofits, and faith-based organizations.
Working
Working outside the home brings with it the very real risk that you will become infected. The primary concern of many workers is that they will become infected on the job and, in turn, infect their family.
To make work safe, we must fund testing and contact tracing, provide protective and sanitary equipment, and create new workspaces that minimize the possibility of transmission.
High-risk and essential workplaces, such as poultry plants, warehouses, grocery stores, child care centers, nursing homes and hospitals, require repeated and random testing for workers who do not appear ill, immediate testing of anyone who has symptoms of the novel coronavirus, and contact tracing for employees, their families, and the public who have come in contact with an employee who has tested positive.
Alabama should use a portion of the $300 million earmarked for the support of citizens, businesses, nonprofits, and faith-based organizations directly impacted by the pandemic or providing assistance to those affected to provide:
- The tests necessary for business and government agencies that have reopened;
- Contact tracing of positive test results;
- Personal protective equipment for employees of those business and government agencies; and
- Increased sanitary stations within essential workplaces.
Alabama also needs to develop or adopt technical assistance on workplace safety detailing how employers test for COVID-19, use PPE, and create safer workspaces.
In exchange for providing these supplies and equipment, Alabama must require businesses to adopt paid sick leave requirements for all employees to protect other employees and the public from transmission of the virus and allow employees to get tested without fear of losing their jobs.
When allocating these funds, Alabama should prioritize supporting minority-owned and woman-owned local businesses and provide small business loans or grants to these businesses to retain employees or make workplaces safer. Minority-owned businesses received fewer Small Business Administration loans under the CARES Act, and because the business owners have less access to credit, they rely on personal funds more than white-owned businesses to finance their work.[1]
In addition, Alabama should follow Congress’ example and provide a one-time tax rebate to low-income households to assist families who are unemployed and underemployed.
Families
One of the largest hurdles for families who are prepared to go to work is finding affordable and safe child care. Approximately one in four working adults has a child under age 18 and in two-thirds of two-parent families with children, both parents work. However, not every family can afford child care. Low-income families who pay for child care spend around 35% of their income on that care. To ensure parents are able to return to work, Alabama needs to provide child care for low-income families. This includes supporting low-income families by making child care affordable and supporting child care centers that are at risk of closing.
Stable families need stable homes. While Governor Ivey’s April 3 proclamation alleviated the immediate threat of eviction and foreclosure, it does not solve the long-term problem for Alabamians unable to pay rent or mortgages now that the emergency order has expired. Many families will not be able to pay the back rent that has accumulated. About a third of low-income and nearly two-thirds of extremely low-income households in Alabama pay more than half of their income on rent and utilities every month. The total cost of rent support needed in Alabama for the duration of this crisis is estimated at a little over $1 billion.[2]
These families and their landlords urgently need rent relief. To meet this significant need, Alabama must:
- Allocate and leverage Coronavirus Relief Fund money in coordination with other sources of federal and private housing assistance funds; and
- Provide emergency relief, through homeless and other nonprofit agencies, for families at risk of eviction, foreclosure or loss of utility service.
Other states have already taken this important step. Montana used $50 million of the Coronavirus Relief Funds it received to provide tenant and homeowner relief. The Pennsylvania Legislature reserved $150 million for emergency rental assistance from its federal funding. Likewise, Illinois allocated $396 million of its funds for housing assistance. It reserved $100 million specifically to meet the needs of people in disproportionately impacted areas based on COVID-19 cases and $79 million for counties that did not receive direct allotments from the federal Coronavirus Relief Funds. Alabama needs to take similar steps to protect its families who rent.
These solutions do not address the overwhelming need for more affordable housing in Alabama. To address this long-term goal, Alabama needs to increase its stock of affordable housing by funding the Housing Trust Fund administered by the Alabama Department of Economic and Community Affairs.
As more Alabama families lose jobs or work hours, hunger is growing in the state. In the last week of May, the Census Bureau’s Household Pulse Survey found that over 10% of Alabama households are experiencing food insecurity–a significant increase from the first week of the crisis. Therefore, we must greatly increase our support to Alabama-based food banks that provide emergency food to hungry families.
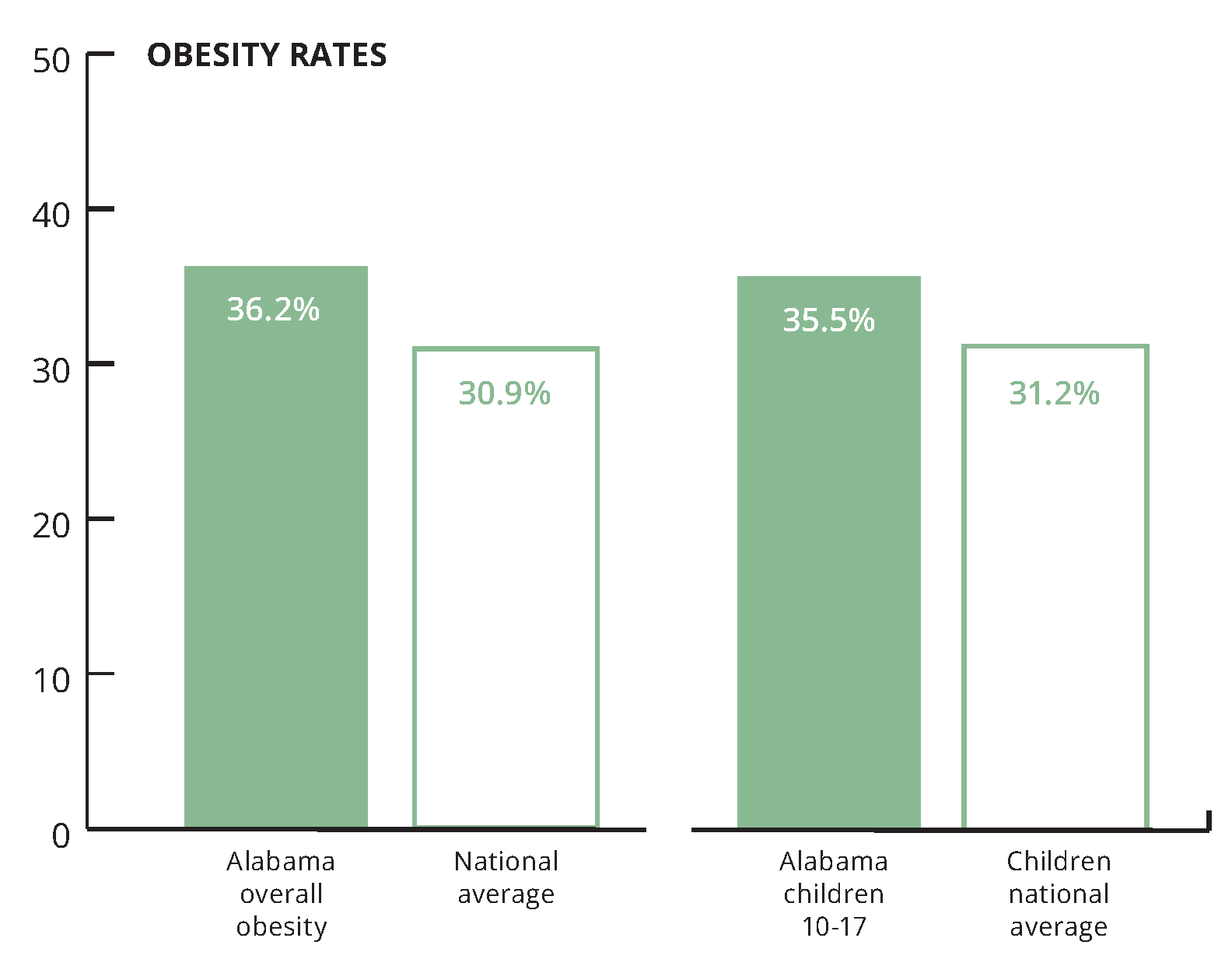
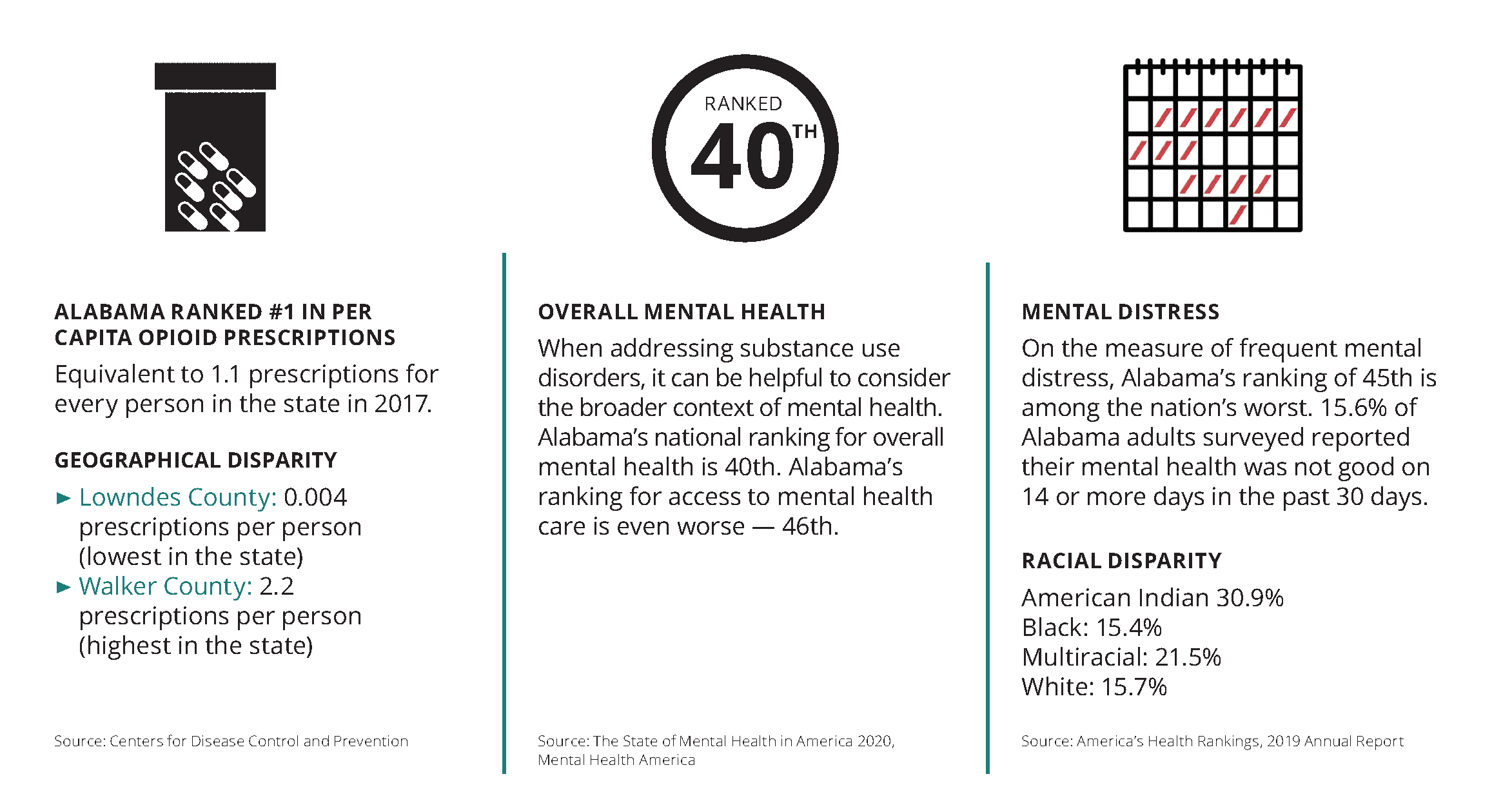
Improving Alabama’s health
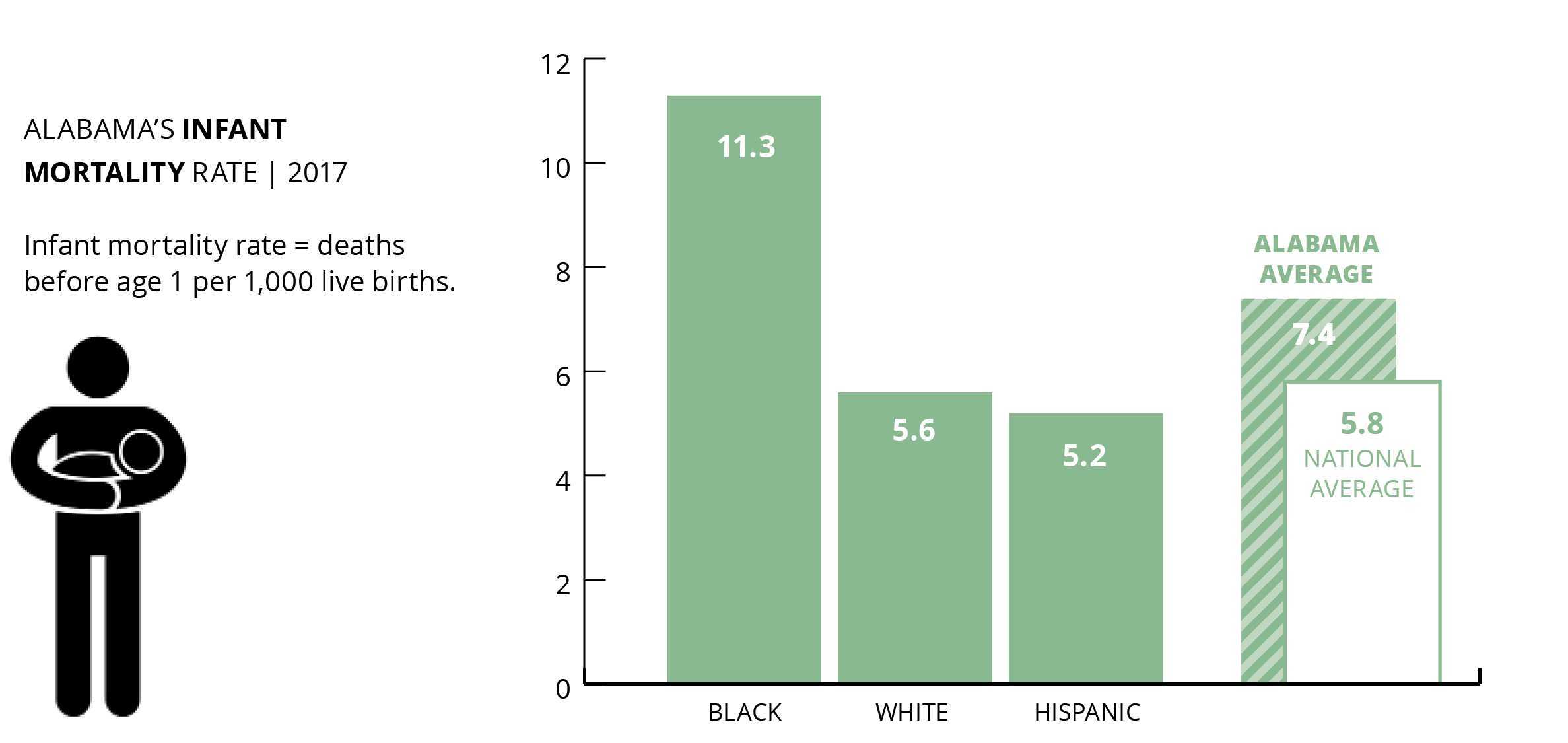
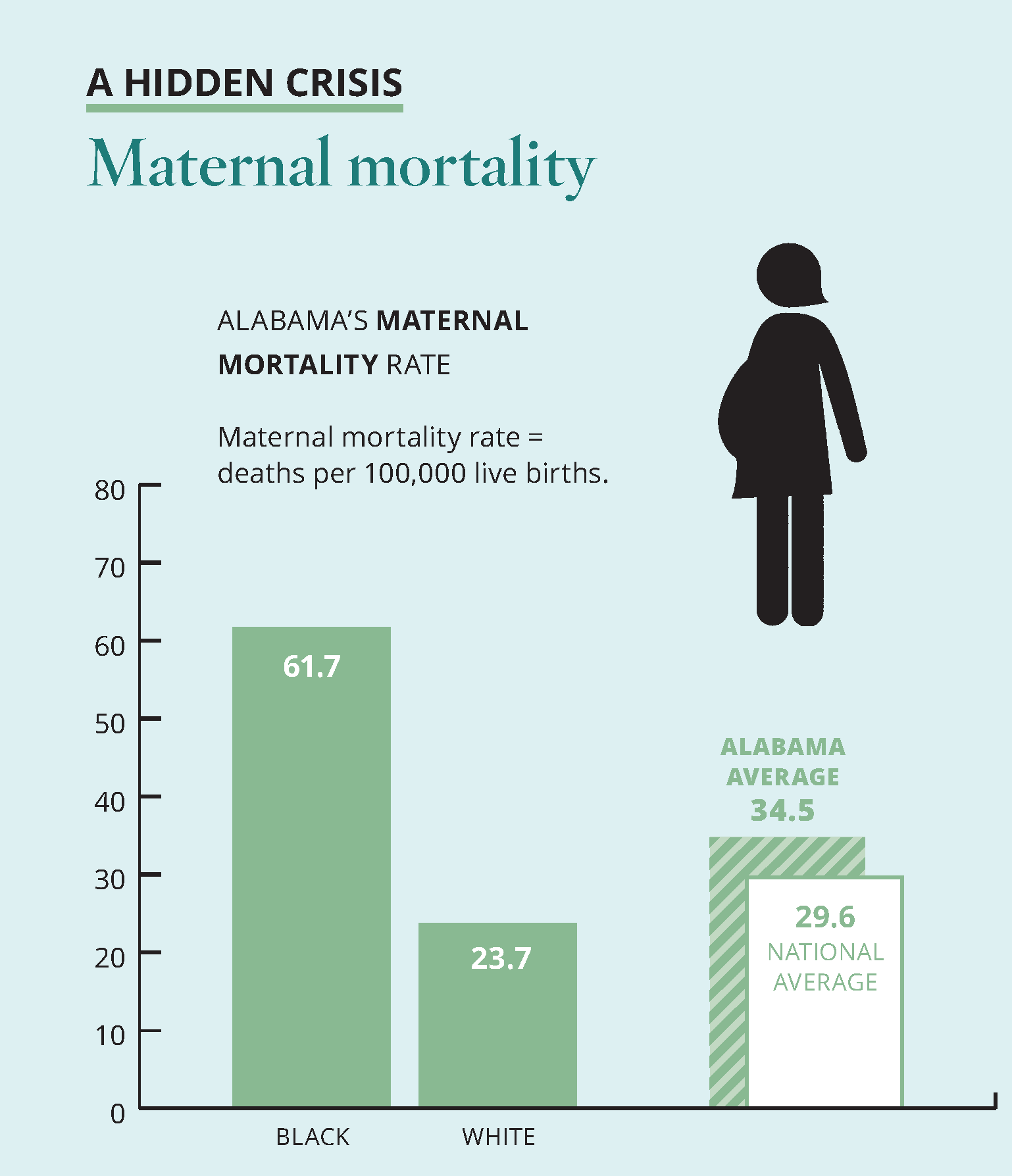
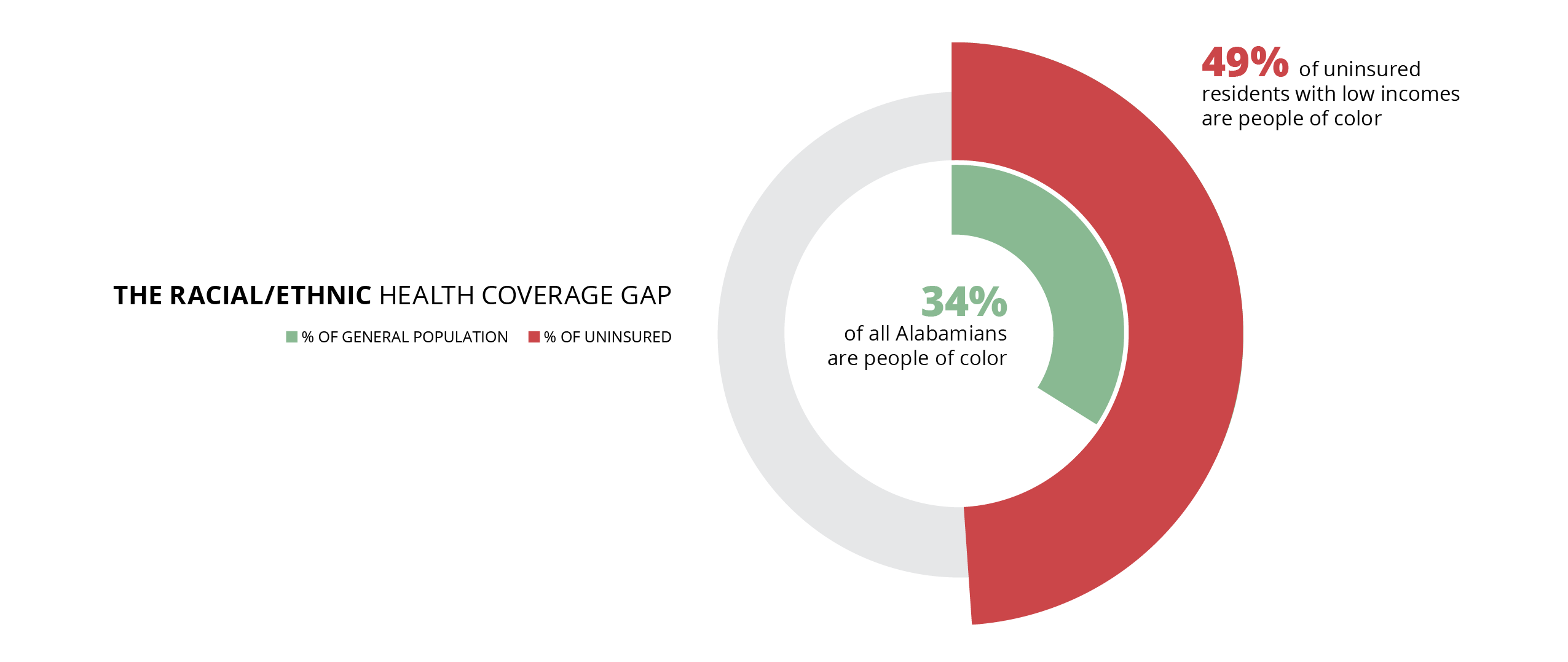
COVID-19 is exposing chronic and deadly inequities in Alabama’s health care system. The virus’s disproportionately high mortality rate for African Americans reflects deep structural barriers to health care, economic opportunity, transportation, and other assets of the common good. These same barriers have impeded the state’s response to the pandemic by limiting the delivery system for mitigation, testing, and treatment in historically underserved communities. In light of these challenges borne of both active exclusion and passive neglect, Alabama’s COVID-19 response should prioritize interventions that explicitly address health disparities.
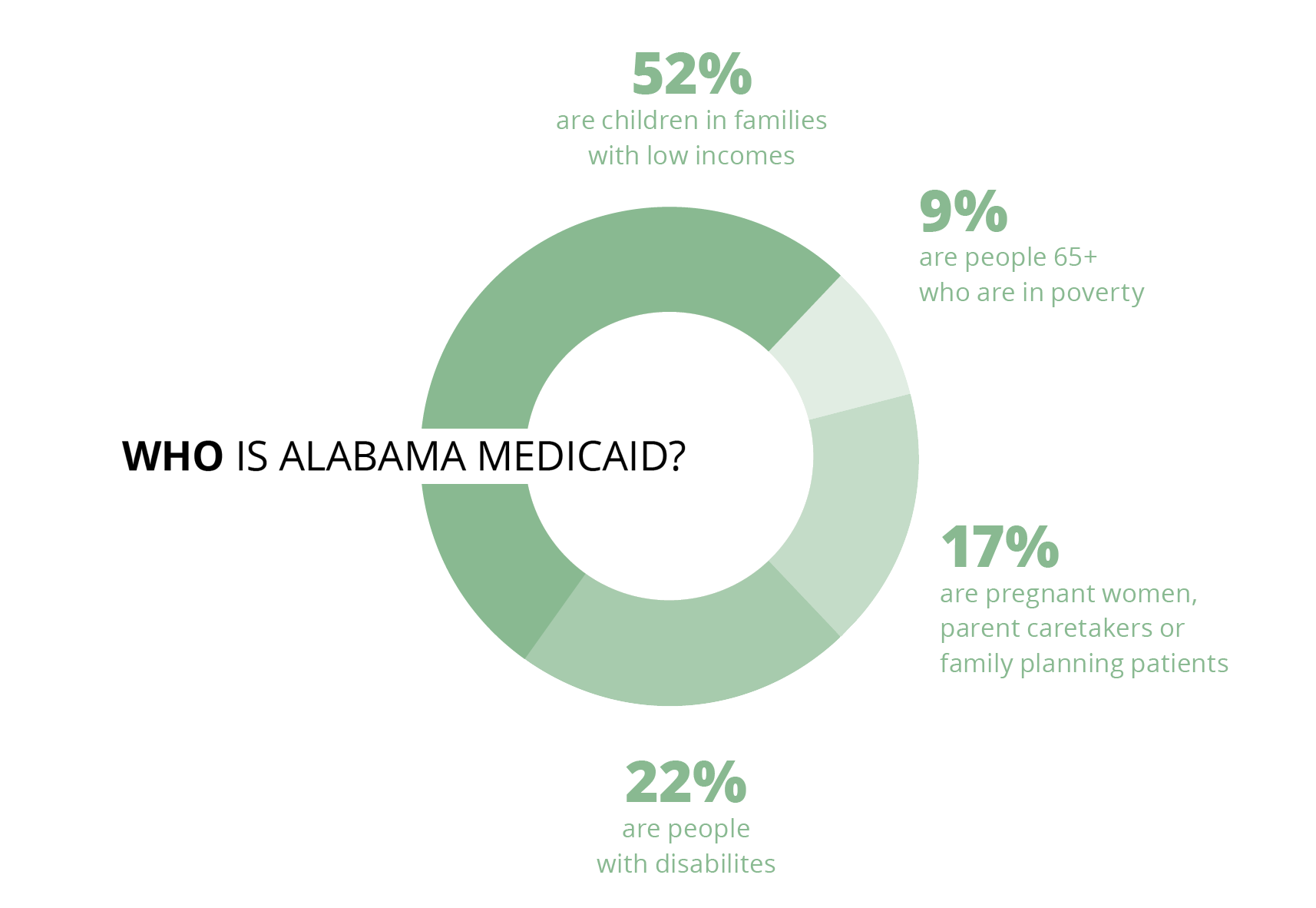
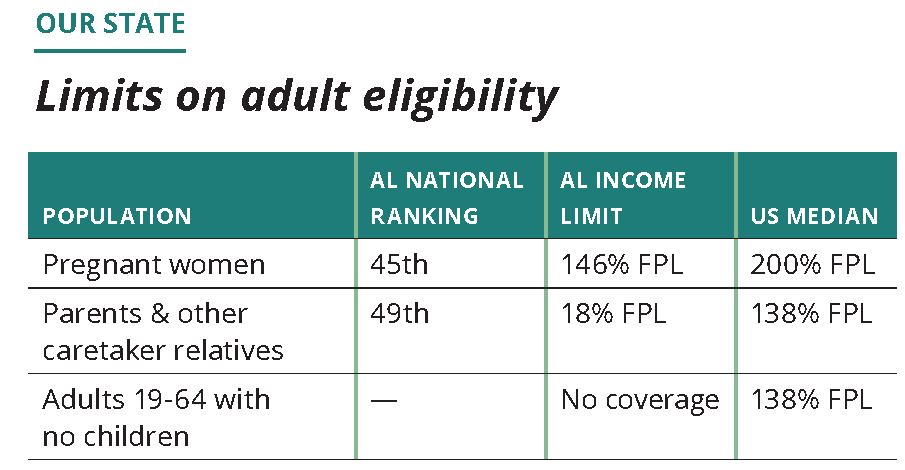
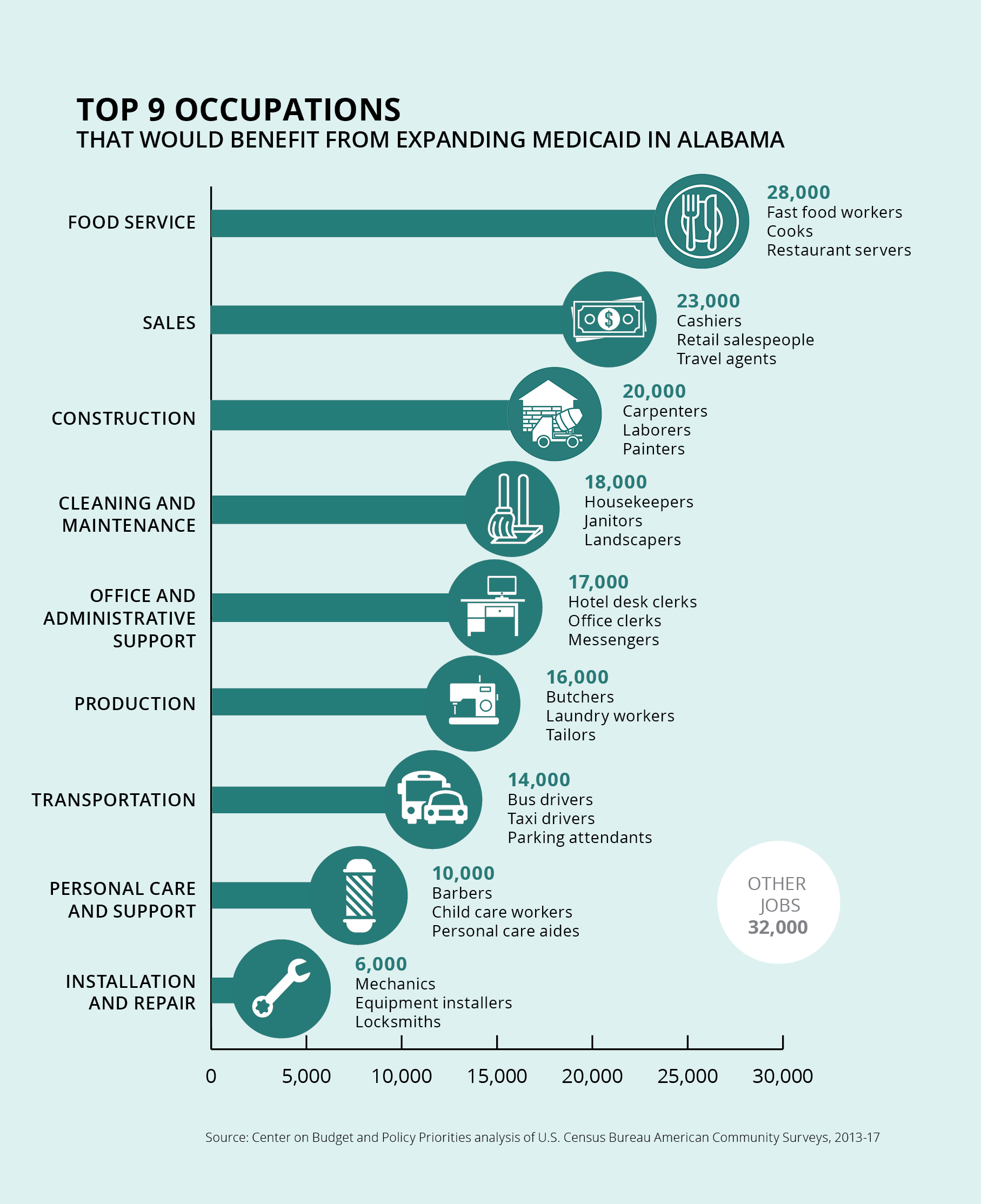
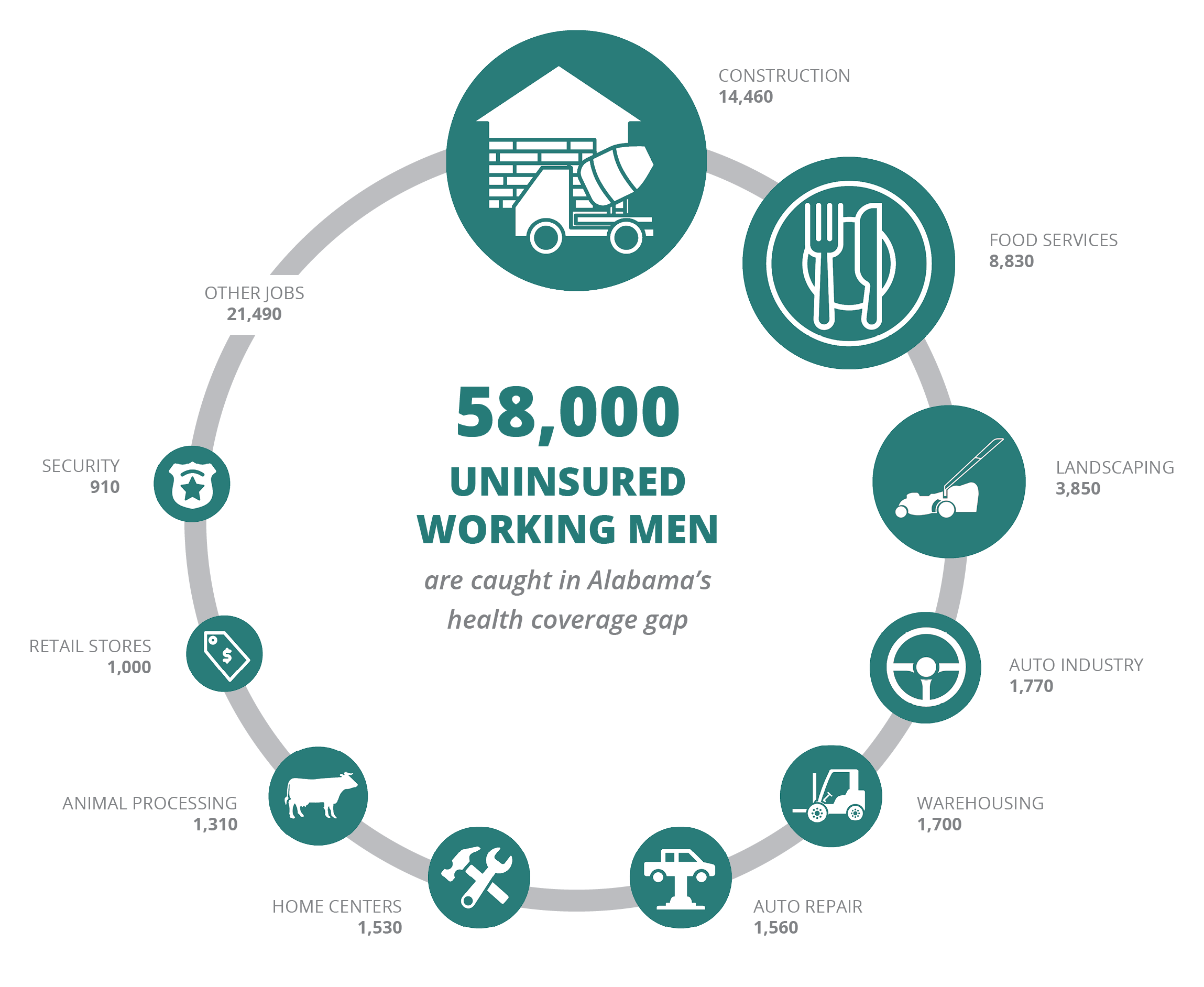
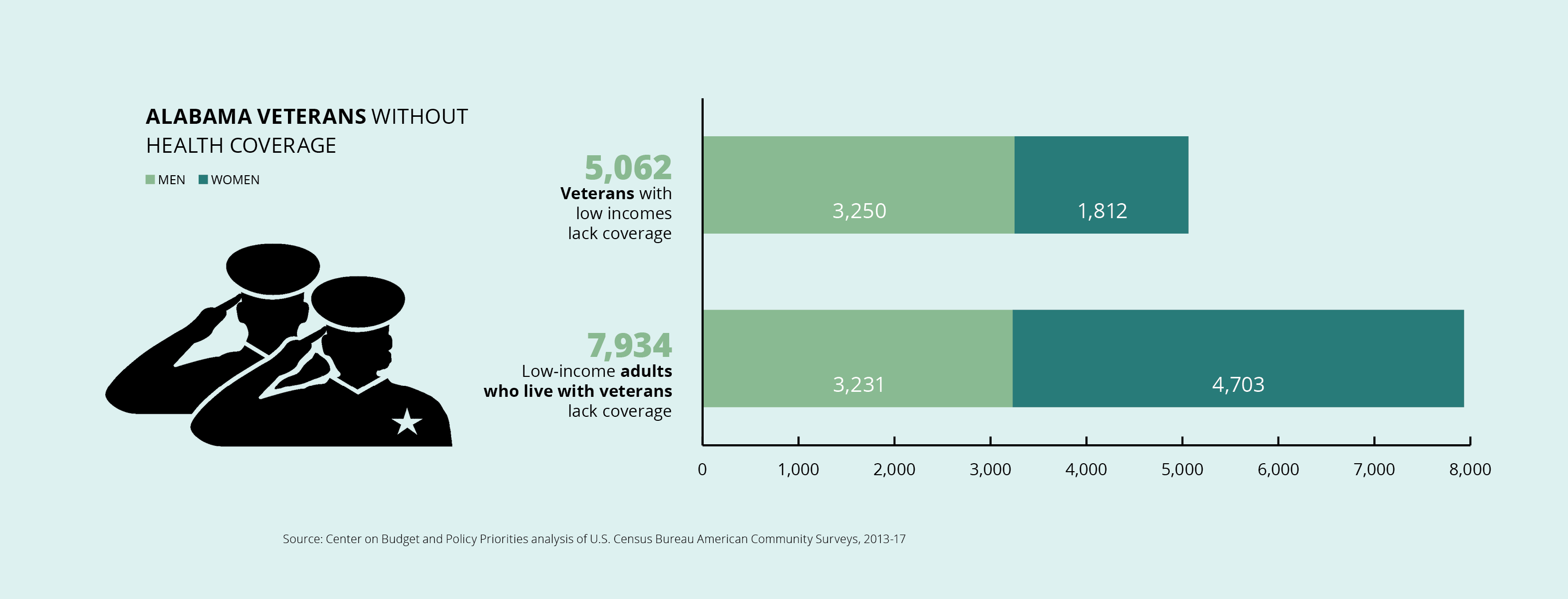
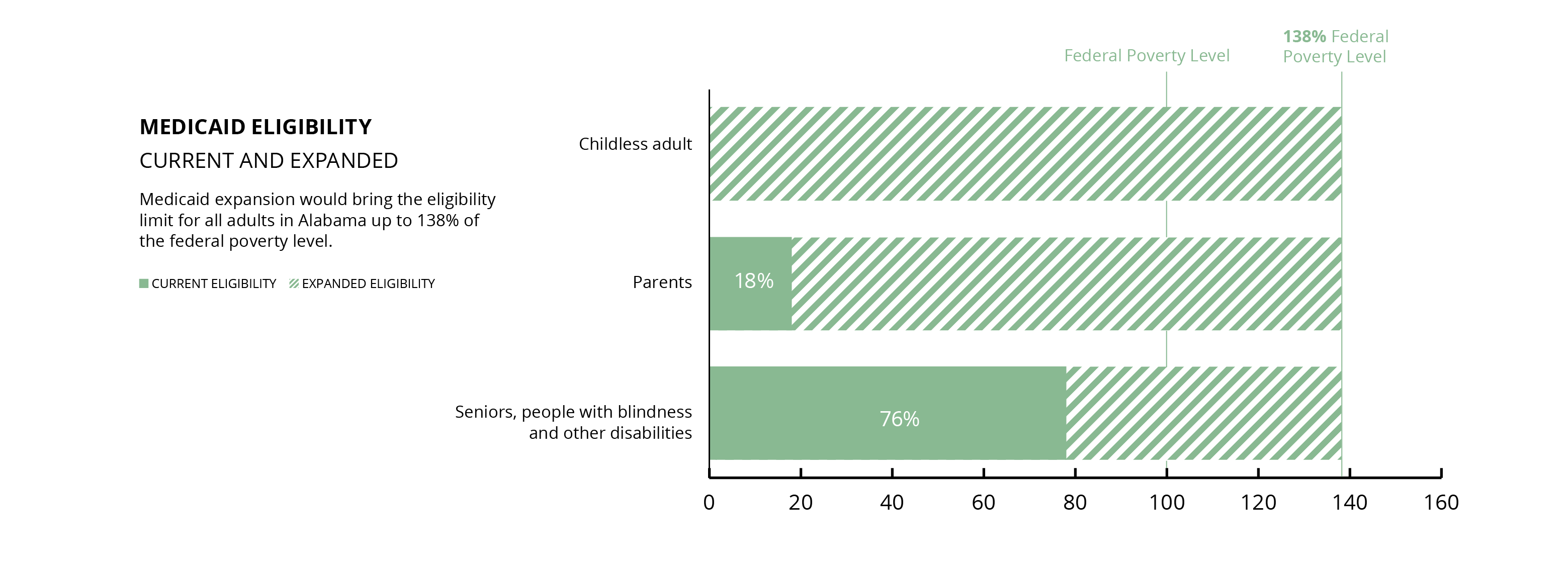
Allocation of federal COVID-19 relief funds does not occur in a vacuum. These funds will have their biggest impact when they flow through or alongside state programs designed to provide basic protections for all Alabamians. The single biggest action Alabama can take to maximize the impact of current and future federal COVID-19 relief funding on historic health disparities in our state is to expand Medicaid. Lack of health coverage for low-income adults creates an “outsider class,” distancing many of our most vulnerable neighbors from emergency resources that could buffer the pandemic’s toll. We recognize that the state cannot use COVID-19 relief funding for the state share of expansion costs.
Thus far, Alabama has set aside $5 million to support the Department of Health and an additional $250 million to support delivery of health care and related services related to the pandemic. Alabama should use these funds to:
- Ensure that there is adequate testing for new infections, including funding for testing supplies;
- Provide contact tracing after new infections are discovered;
- Supply PPE to areas that have been most impacted by COVID-19; and
- Strengthen public health surveillance systems to facilitate rapid response to local infection upsurges as economic activity increases.
Adequate testing for the virus is the most urgent tactical need. A primary tool for targeting finite (and admittedly inadequate) resources is accurate information. The state must evaluate the extent and adequacy of testing in each Public Health District in order to prioritize additional resources for underserved districts and facilitate partnerships between local health departments, private testing providers and local community and faith groups to ensure assistance for all who need it.
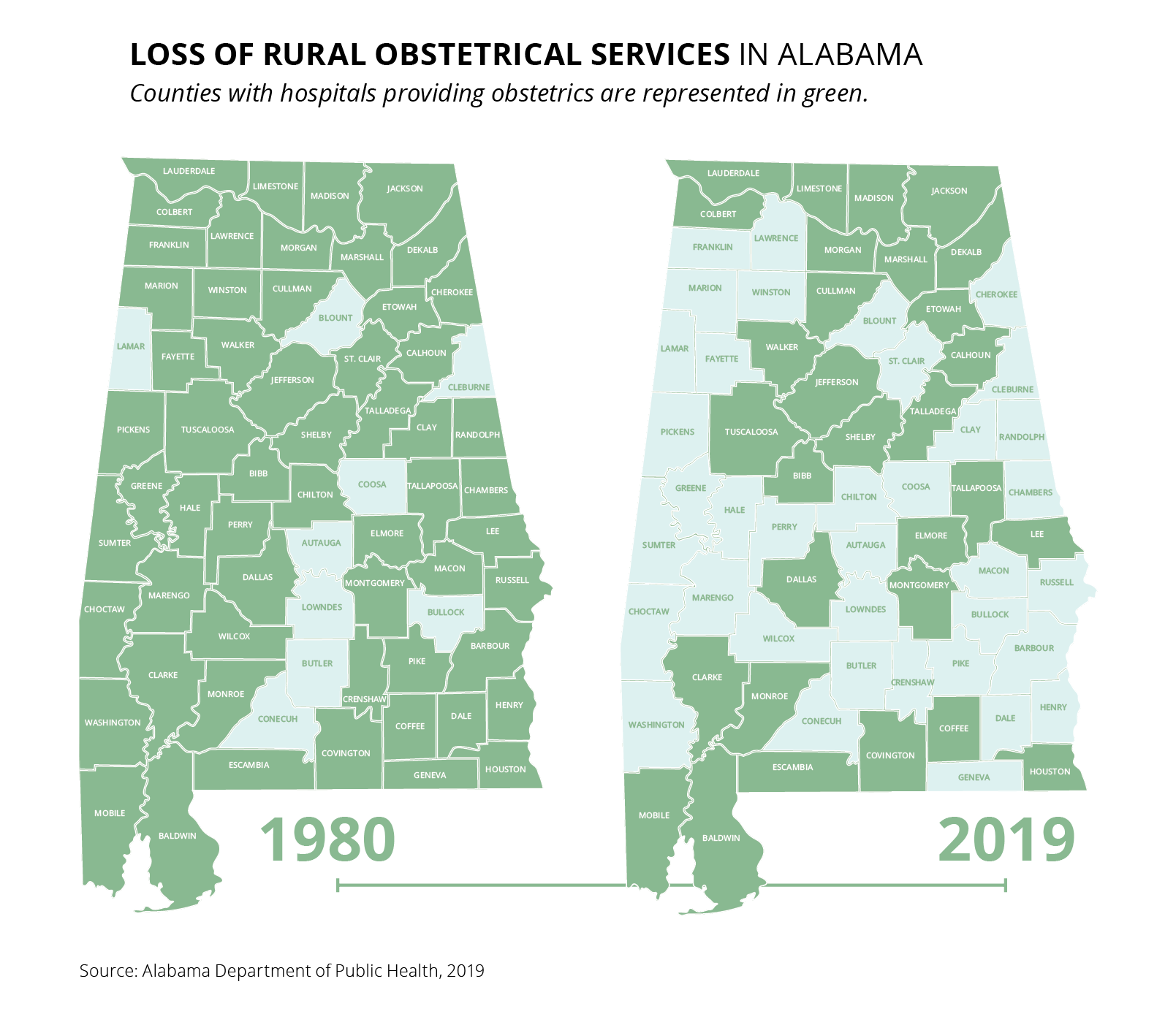
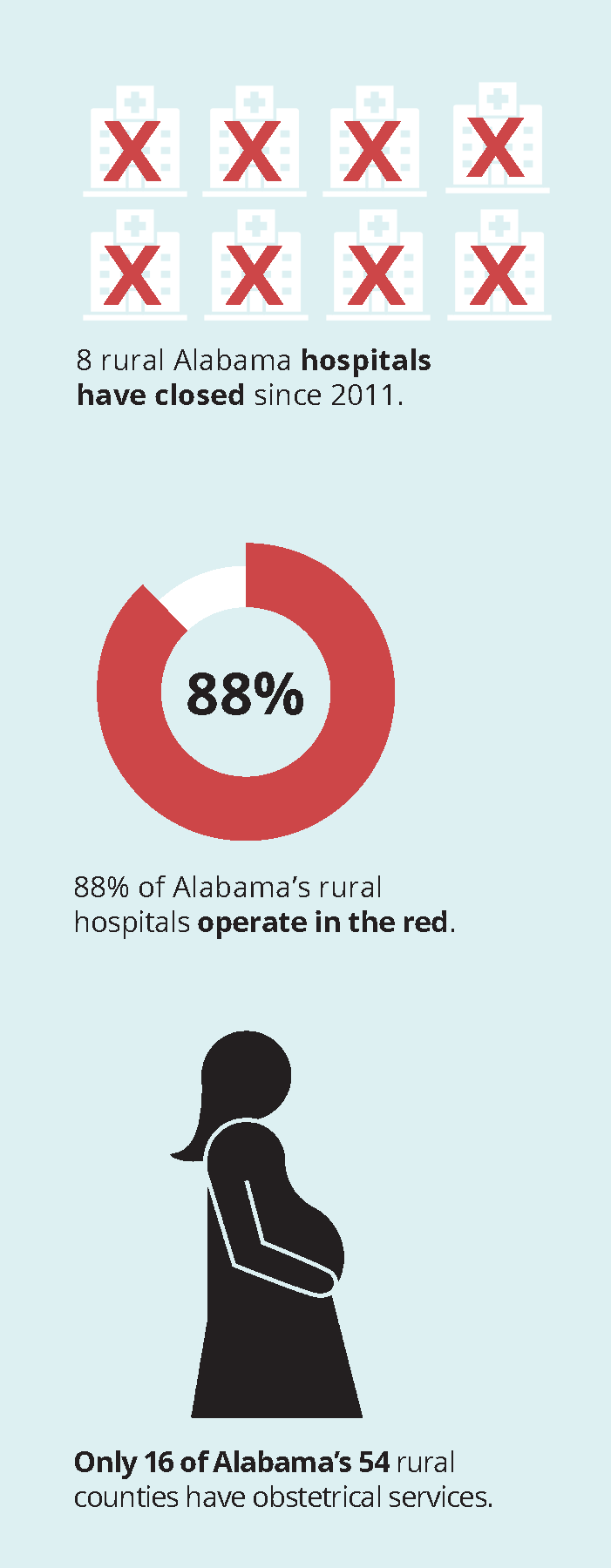
Another barrier to both testing and treatment is lack of transportation, especially in rural areas. To address this concern, Alabama should appropriate a portion of COVID-19 relief funds to the Public Transportation Trust Fund to mitigate coronavirus-related drops in local agencies’ farebox recovery rates.
Safely reopening state and local services
Reopening our courts
The Alabama Supreme Court has authorized the presiding circuit judge in each circuit to continue court closures until August 15 for all courts within the circuit, including municipal courts, to preserve the safety and welfare of court personnel and the public. We would encourage delaying non-essential hearings for as long as possible, so long as the delays do not affect the rights of litigants. However, when courts reopen, they will need to take special precautions to protect people with disabilities or with family members who are vulnerable to infection. Funding to courts should require that they develop, and make accessible, a comprehensive reasonable accommodation policy for civil and criminal cases that addresses the individual needs of lawyers, litigants, defendants, and witnesses who cannot physically come to court due to disability.
These accommodations could be as simple as continuances or remote video proceedings for people who have access to technology necessary to participate in the proceedings remotely. If remote proceedings are used, funding should be used to allow for technology that permits video to enhance credibility determinations by fact finders, that allows the introduction and viewing of documentary evidence by remote participants, and that provides access, or education about the requisite technology for participants prior to their hearing.
Alabama also should increase funding to support ADA coordinators within courts that individuals with disabilities can contact in the event that an accommodation is needed.
In addition to delaying court reopenings and taking necessary steps to protect people with disabilities, a portion of the $10 million set aside for court services should fund personal protective equipment for all people required to attend court functions, including court personnel, attorneys, witnesses, victims, and litigants. Additionally, a portion of those same funds should be used to promptly notify individuals with court dates of delays, cancellations, and rescheduled hearings. Not only should these notices be sent to individuals, but as the hours and operating conditions of the courts evolve and change, the court should ensure that the public is aware of current court policies and how people seeking emergency relief may access the courts. These notices should be prominently posted at the courthouse, online, and in any other location likely to inform the public.
Improving state services
The pandemic caused a groundswell of need for services administered by Alabama, including the Supplemental Nutrition Assistance Program (SNAP), Medicaid, Temporary Assistance for Needy Families, Unemployment Insurance benefits, and subsidized housing programs (which are primarily run at a local level). As more residents need these supports to make it through the pandemic, Alabama should prioritize the $300 million it has set aside for state agencies to increase the numbers of case handlers they employ to respond to the increased demand, provide those workers with resources they need to work from home or with the same testing and PPE that we recommend for all essential workers when they engage with the public, and collectively improve access to their services using mobile technology.
When an individual is going through a crisis or the entire state is in a pandemic, these disparate services need to be accessible in one place with minimal barriers to applying for benefits, receiving important correspondence about deadlines or reporting obligations, and communicating with case workers about the services. Applying and maintaining these services comes at a high opportunity cost to families. Currently, to apply for and communicate about each service takes hours, often at different agencies and with different case workers. That is time that people need to take care of their children, their elderly parents or neighbors, or to look for employment. Improving capacity and access now both responds to the current crisis and inoculates these agencies for future crises.
Voting
In addition to improving access to state services, Alabama must protect our citizens’ health and fundamental right to vote. A portion of the $300 million set aside for state services should be used to provide absentee ballot applications to every registered voter or, at a minimum, allow every registered voter to request and vote by absentee ballot during the pandemic. In addition, because many voters require or prefer in-person voting, the state must work to improve the safety and accessibility of in-person voting and permit curbside voting. To ensure voters know how to vote safely during the COVID-19 pandemic, Alabama will need to increase its spending to educate voters in coordination with local election officials.
Taking responsibility for people in our custody
Alabama has both a legal and a moral responsibility for the safety and well-being of the people it incarcerates. There are tens of thousands of individuals housed in state prisons, local jails, and ICE detention facilities — all places where it is impossible to practice social distancing. To date, less than 1% of those incarcerated in Alabama’s prisons have been tested for COVID-19.
Governor Ivey with approval from the Legislature has set aside $200 million for the Department of Corrections to help meet Alabama’s moral and legal obligations during this pandemic. We recommend that Alabama prioritize its use of the funds to:
- Release all incarcerated people who do not pose a threat to public safety, who are pregnant, and people who are at a higher risk if infected with COVID-19;
- Assist with reentry services to enable successful reintegration for returning persons;
- Test people in Alabama jails and prisons prior to release and while incarcerated; and
- Provide PPE, soap, sanitizer, and other supplies necessary to maintain a safe and hygienic environment for the remaining incarcerated people and correctional staff.
The fastest way to reduce the threat of infection in jails and prisons is to test and release as many people as possible to reduce the number of people within the facilities. However, decarceration requires more than releasing someone from jail or prison. We also must prioritize a successful reentry into communities to prevent recidivism. A portion of the funds allocated for the Department of Corrections must go to increasing reentry services to ensure successful and safe transitions into the community. Particularly important to this transition are ensuring that people are tested for the coronavirus before reentering and that they are provided with the housing, employment, and medical services necessary once they are in the community. Some states have reduced their populations by nearly 20%. Alabama must do more.
In addition to expediting reentry and funding reentry services, Alabama needs to ensure that people are not set up to fail with onerous fines and fees used to fund the criminal justice system and reentry monitoring. Unemployment is already at record highs, and we know that the effects of racial bias in the hiring process increase the already negative effects of criminal records for people of color. Studies have shown that Black applicants with a criminal record had only a 5% chance of receiving a call back, less than one-third of white applicants with a criminal record. Reentering into this economy will be tough. Having paid for reentry with federal funds, Alabama should waive the fines and fees for people who are struggling to reintegrate into our communities, giving them a clean start and a better chance for success.
Even with fewer people in facilities, we will still need to dramatically increase testing of employees who work in prisons and jails and for the people who are incarcerated therein. Only four in every 100 residents in Alabama have been tested for COVID-19. Alabama has tested fewer than 1% of people incarcerated in its prisons. This is wholly inadequate to slow, let alone stop, the spread of COVID-19 within Alabama’s facilities.
Securing our children’s futures
The pandemic radically impacted education and threatens to worsen future education outcomes in Alabama for the many students who already did not have the benefit of an equitable opportunity to learn before it began. Alabama must focus its attention on addressing the inequities exacerbated by access to technology, space to learn, and caretakers to support their learning and those for whom specialized services are not available, including for students with disabilities. If it does not, the opportunity gap will widen with significant economic impacts for students and their families far into the future.
The opportunity gap experienced by low-income children and children of color begins early in life. We must intervene and use a portion of the dedicated $300 million for expenditures related to technology and infrastructure for remote instruction and learning to provide support to organizations offering early intervention programs for at-risk children so that these services can be provided safely and, as necessary, remotely.
Alabama also should prioritize the use of the $300 million to fund public schools with the highest proportion of students who are low-income children, children of color, children with disabilities, English-language learner children, children in immigrant families, children in foster care, migrant children, children experiencing homelessness, LGBTQ children, and children in the juvenile justice system. Public schools likely will need to hire additional staff, including counselors, to provide necessary education, social and emotional, and health and safety services and increase salaries to remain competitive for educators who now take greater risks to their own health and are required to master more technological skills to teach their kids.
We recognize that the $300 million allocated by the Legislature will not be enough. Additional funding could also be taken from the $250 million fund for local government expenditures directly related to the pandemic to provide these disproportionately affected school systems and their local communities with funding for after-school, summer school, and community programs for youth.
Finally, where there are competing priorities for funding, the Legislature has set aside an additional $118 million that can be used to supplement the funds required for these recommendations. If you have any questions or concerns about any of these recommendations, please contact Robyn Hyden (Robyn@alarise.org or 334-832-9060) or Katie Glenn (katie.glenn@splcenter.org or 334-531-7638).
Signatories
Sincerely,
90 Alabama organizations
ACLU of Alabama
Adelante Alabama Worker Center
AIDS Alabama
AL CURE
Alabama Appleseed
Alabama Arise
Alabama Black Women’s Roundtable
Alabama Civic Engagement Coalition
Alabama Coalition for Immigrant Justice
Alabama Coalition on Black Civic Participation
Alabama Faith Council
Alabama Institute for Social Justice
Alabama Justice Initiative
Alabama NAACP
Alabama Poor People’s Campaign
Alabama Rivers Alliance
Alabama Solutions, A Grassroots Movement
Alabama Youth and College NAACP
Amalgamated Transit Union Local 770
Auburn Unitarian Universalist Fellowship
Baptist Church of the Covenant
Bay Area Women Coalition, Inc.
Beloved Community Church
Birmingham AIDS Outreach (BAO)
Children First Foundation, Inc.
Christian Church in Alabama-Northwest Florida
Christian Methodist Episcopal Church
Church of the Reconciler, UMC (Birmingham)
Church Women United Montgomery
Citizens’ Climate Lobby – Baldwin County, Alabama Chapter
Collaborative Solutions, Inc.
Etowah Visitation Project
Fairhope Unitarian Fellowship
Faith and Works Statewide Civic Engagement Collective
Faith in Action Alabama
Fall Injury Prevention And Rehabilitation Center
First Christian Church – Disciples of Christ (Montgomery)
First Congregational Church, UCC (Birmingham)
Five Horizons Health Services
GASP
Greater Birmingham Ministries
Hispanic Interest Coalition of Alabama
Holiday Transitional Center
Holy Rosary Catholic Church
Human Rights Campaign Alabama
Humanists of North Alabama
Immanuel Presbyterian Church, PCUSA (Montgomery)
Interfaith Montgomery
Jesuit Social Research Institute
Jobs to Move America
Just Faith, Prince of Peace Catholic Church (Birmingham)
Just Faith, Our Lady of the Valley Catholic Church (Birmingham)
League of Women Voters of Alabama
Low Income Housing Coalition of Alabama
Macedonia Missionary Baptist Church (Daphne)
March of Dimes
Mary’s House Catholic Worker
Medical Advocacy & Outreach
Mission Possible Community Services, Inc.
Monte Sano United Methodist Church
Montevallo Progressive Alliance
Montgomery Pride United
National Action Network – Birmingham Chapter
National Lawyers Guild
National MS Society
Nightingale Clinic
North Alabama Conference United Methodist Women
North Alabama Peace Network
Open Table United Church of Christ
People First of Alabama
Planned Parenthood Southeast
Progressive Women of Northeast Alabama
Project Hope to Abolish the Death Penalty
Restorative Strategies, LLC
Saint Junia United Methodist Church
Shelby Roden, Attorneys at Law
Sierra Club, Alabama Chapter
Sisters of Mercy Alabama
Sisters of Mercy of the Americas
Southern AIDS Coalition
SPLC Action Fund
St. Andrew’s Episcopal Church (Birmingham)
The Empowerment Alliance
The Green Kitchen
The Right Place, Inc.
The Women’s Fund of Greater Birmingham
Unitarian Universalist Fellowship of Mobile
URGE: Unite for Reproductive & Gender Equity
Yellowhammer Fund
Youth Towers
YWCA Central Alabama
cc: Governor Kay Ivey and policy staff
[1] The SBA Inspector General found that the SBA failed to instruct lenders to prioritize underserved and rural markets [found at https://www.sba.gov/sites/default/files/2020-05/SBA_OIG_Report_20-14_508.pdf on May 27, 2020]. Disparities in lending between minority-owned and white businesses already existed as documented by the Federal Reserve Bank of Atlanta’s December 2019 Small Business Credit Survey [found at https://www.fedsmallbusiness.org/medialibrary/fedsmallbusiness/files/2019/20191211-ced-minority-owned-firms-report.pdf on May 27, 2020].
[2] Estimate from the National Low Income Housing Coalition.







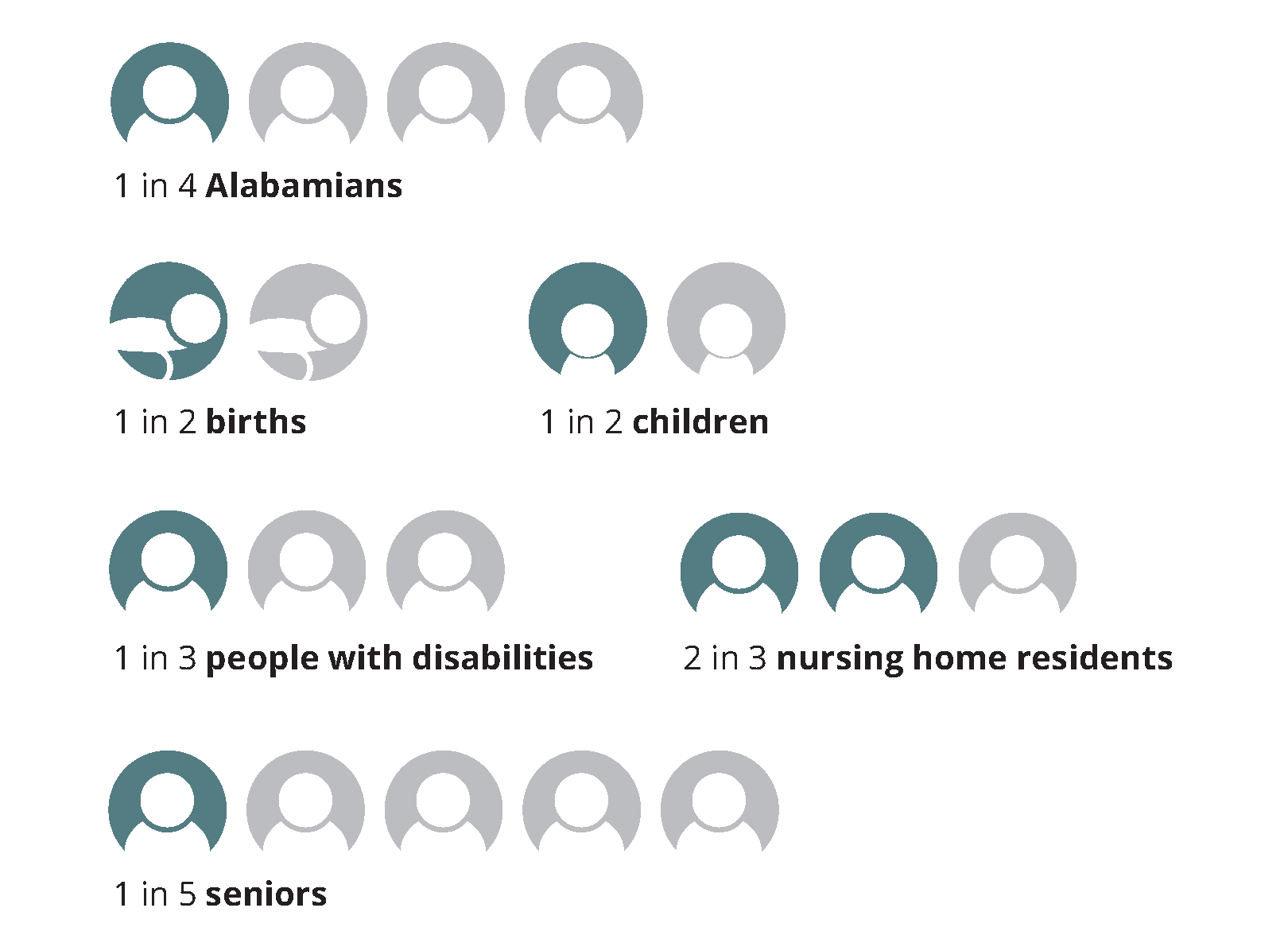
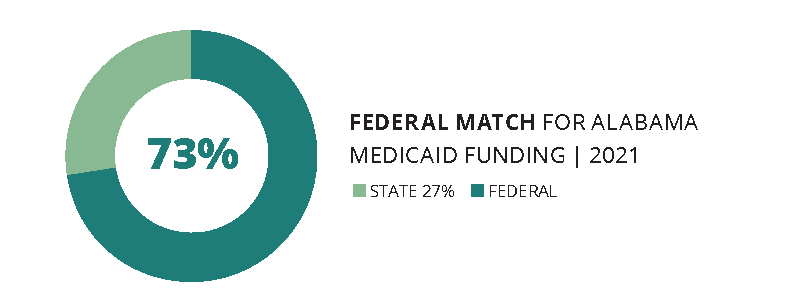
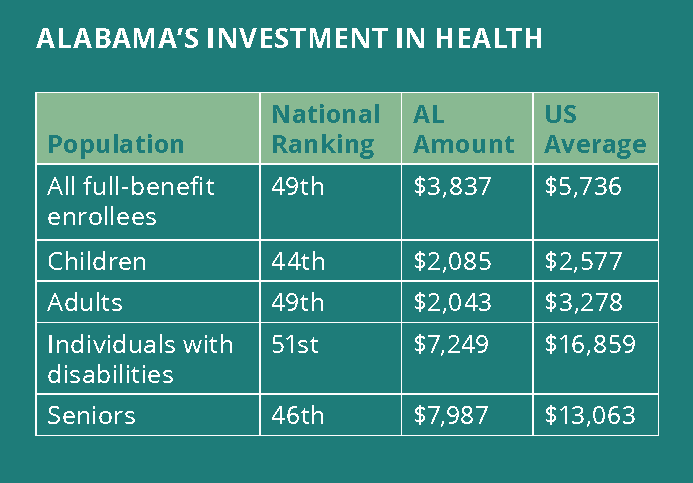
 Medicaid pumps $7 billion in federal and state money into our health care system every year. Without Medicaid funding, many of the doctors’ offices, clinics, hospitals and other medical facilities that all Alabamians depend on would have to cut services or close.
Medicaid pumps $7 billion in federal and state money into our health care system every year. Without Medicaid funding, many of the doctors’ offices, clinics, hospitals and other medical facilities that all Alabamians depend on would have to cut services or close.