The following is a joint statement from Alabama Arise, the Alabama State Conference of the NAACP and Greater Birmingham Ministries:
Our elected officials and appointed leaders should respect the full dignity, worth and humanity of all people they represent. We urge all political parties and public officials to acknowledge the harm that white supremacy continues to inflict upon Alabama. And we call upon them to dismantle white supremacist structures through intentional policy changes.
The cause of white supremacy permeates our state’s fundamental governing document. When the president of the 1901 constitutional convention, John Knox, was asked why Alabama needed a new constitution, his answer was clear: “to establish white supremacy in this state.”
Any celebration of Nathan Bedford Forrest of the Ku Klux Klan – a white supremacist terrorist organization – is contrary to the values that Alabamians expect from our leaders, elected officials and neighbors. In celebrating Forrest, Rep. Will Dismukes revealed he is unable or unwilling to represent the best interests of his constituents and his state. We condemn his actions in the strongest possible terms. We also understand this is not the first time Dismukes has celebrated the Confederacy or Forrest in such a manner. Therefore, we join with many other individuals and organizations across Alabama in calling for Dismukes to resign immediately.
Racial equity requires action, not just words
Alabama’s need for racial justice and healing reaches far beyond any one individual. All elected officials must take a hard look at both their actions and the impacts of their policy decisions. Most lawmakers claim to support racial equality, but the results of their policy choices often do not match this claim.
Examples of this mismatch are unfortunately common in our state. The 2017 Memorial Preservation Act prevents localities from removing statues that “honor” the Confederacy without paying a steep fine or getting approval from a panel of legislators that to our knowledge has not approved a removal since the law was enacted. Lawmakers’ failure to expand Medicaid leaves a disproportionate share of African Americans without health insurance during a pandemic. And the absence of racial impact data prevents communities and legislators from evaluating the full effects of state policy choices.
The harsh reality of racial disparities in Alabama
While Dismukes dismisses the need for racial reconciliation in today’s society, we cannot remain ignorant of the truth. We all must reckon with these disparities created and maintained by structural policy barriers:
Black children are nearly three times as likely as white children in Alabama to grow up in poverty. That is true even though the labor force participation rate among Black workers is equal to that among white workers. This disparity is the result not of individual failures but of systemic and structural failures.
Historically inequitable tax structures privilege large landholders and prevent schools serving Black students in rural Alabama from raising adequate revenues. These tax structures created a pattern of “unequal and inadequate public school funding,” according to a 2011 U.S. District Court ruling in Lynch v. Alabama.
Black people are twice as likely as white people to be locked up in Alabama jails. And they are nearly three times as likely to end up in Alabama prisons. Abundant research shows discriminatory policing and sentencing, criminalization of poverty and unequal access to counsel are key drivers of these incarceration disparities.
It’s time for more than talk. Denouncing and rejecting white supremacy is only the beginning. Lawmakers also must enact meaningful policy changes to break down institutional barriers to opportunity and justice for all Alabamians.
Many Alabamians have modified their work circumstances in recent months to reduce the risk of contracting COVID-19. But tens of thousands of people still must work in public-facing jobs that put them at increased risk of illness.
Front-line workers in grocery stores, hospitals and pharmacies perform necessary tasks to keep our communities functioning during the pandemic. The burden of facing those health risks is unevenly distributed, though. Workers in jobs like health care, food service and child care are disproportionately likely to be people of color or women. And state and national policy failures on COVID-19 are more likely to hit them the hardest.
Gender disparities and low wages increase risk
Differing employment levels in the health and retail fields particularly have forced more women to risk coronavirus infection. Two-thirds of Alabama’s essential workers are women, though women comprise just under half of the state’s total workforce.
Health care workers overall are much more likely to be women, and they face drastically heightened risk of infection at work. Among Alabama workers, women comprise 81% of health care workers and 89% of child care and social services workers. Jobs in these fields often require consistent exposure to large numbers of people.
Health care accounts for more than one in 10 jobs in Alabama. And the higher proportion of women in this field contributes to a gender-based disparity for COVID-19 exposure. In many cases, personal protective equipment (PPE) has run short for doctors, nurses and other health care professionals. This structural failure has forced many of these workers to reuse PPE, posing potentially severe health risks.
The wages and work conditions for essential front-line workers often don’t reflect the importance of their work. Many workers received higher hourly wages early in the pandemic, but now some employers have begun eliminating hazard bonuses. In the retail sector – already filled with low-wage jobs with sparse benefits – major employers like Amazon, Kroger and Target have stopped their wage bonuses.
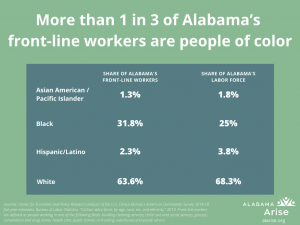
Even among essential workers, people of color are more likely to face heightened exposure in certain public-facing industries. In Alabama, the share of Black people working in grocery or convenience stores is two and a half times larger than in the U.S. workforce overall. The share of Asian Americans and Pacific Islanders who work in grocery and convenience stores is double their percentage of Alabama’s overall population.
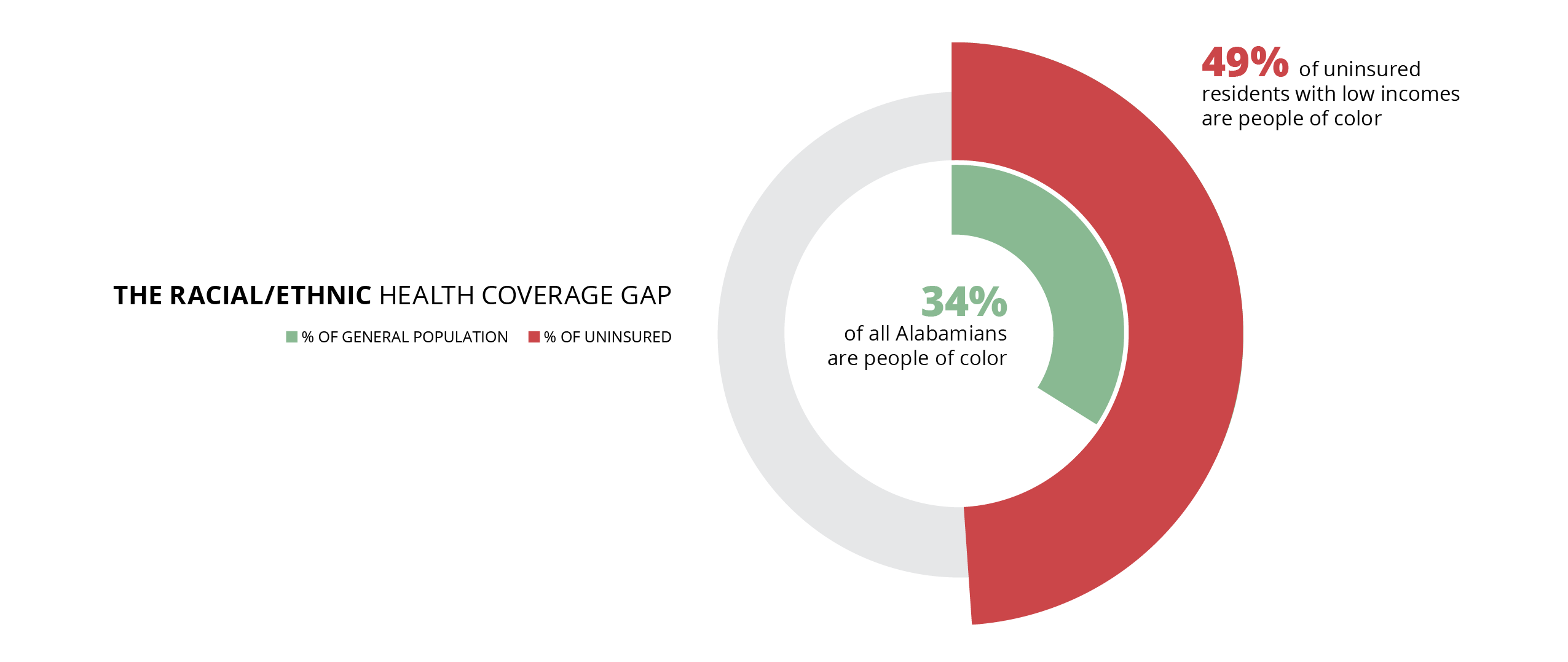
Despite these elevated risks, Black and Latino Alabamians are far more likely than white people to lack health insurance coverage. And because Alabama hasn’t expanded Medicaid, Black and Latino residents are more likely to fall into the health coverage gap, earning too much to qualify for Medicaid but too little to afford insurance. People of color make up 34% of Alabama’s population but comprise 49% of uninsured Alabamians with low incomes.
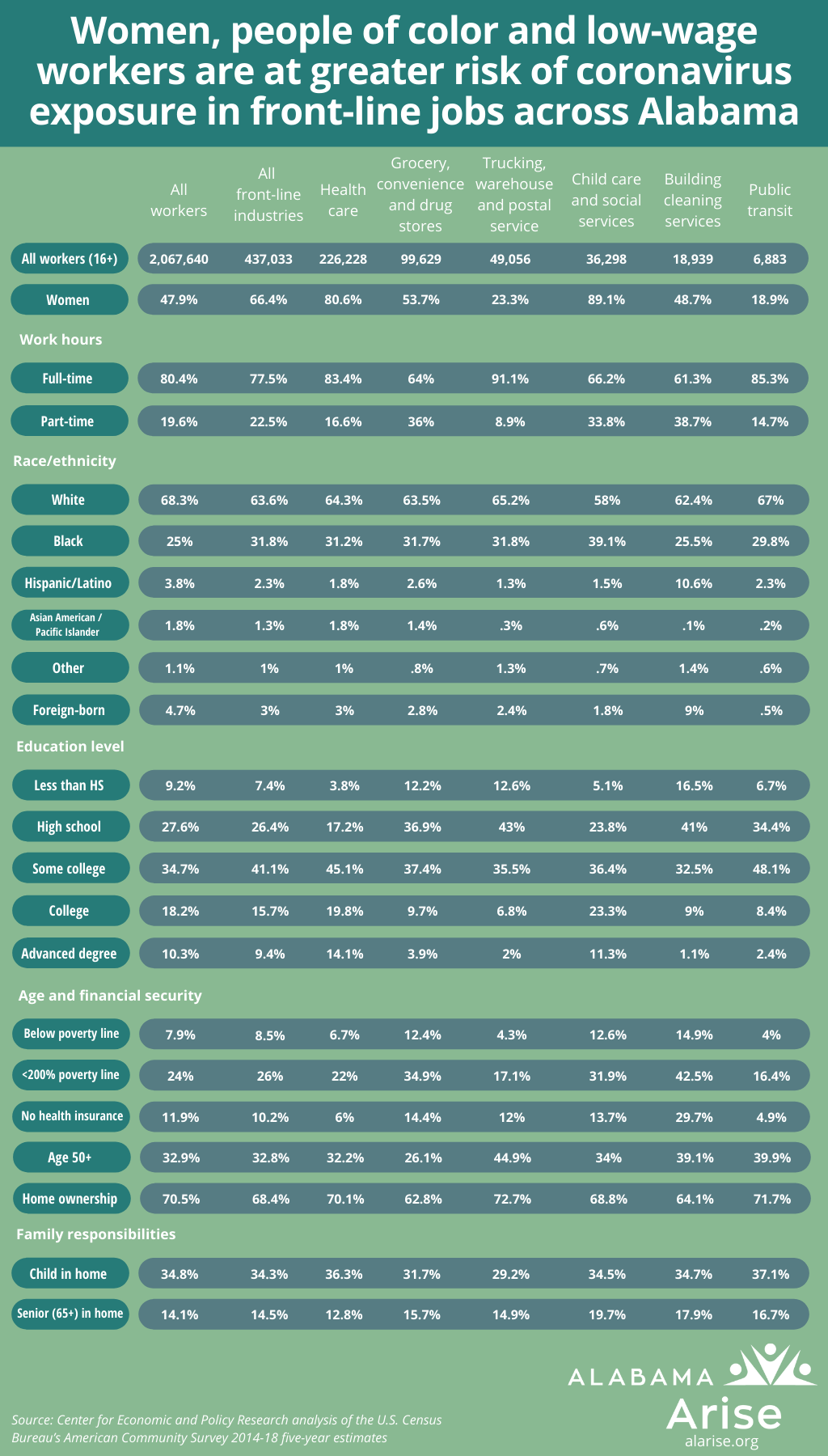
This table shows the disproportionate burden that women, people of color and low-wage workers face across several essential employment fields:
Unfortunately, the chart’s data cannot account for differing exposure rates based on specific jobs within those career fields. But given that women in medical fields often face bias inhibiting their promotion into supervisory roles, women are likely at greater risk of coronavirus infection than their high proportion in the health care industry indicates. And overall, people of color are more likely to work non-supervisory jobs with higher public exposure in many front-line fields.
Shortsighted policy choices harm the economy and virus containment
Refusal to expand Medicaid and attempts to slash UI benefits are harmful policy decisions that fly in the face of the reality of the pandemic. And the burden of these cruel choices falls more heavily on people who already face disadvantages in the labor market.
More than 600,000 people have filed UI claims in Alabama since the pandemic reached the state in March. Thousands of Alabamians are already losing UI benefits for refusing to return to work in conditions they see as unsafe. Each person prematurely knocked off the UI rolls loses not only the $275 monthly state benefits, but also the $600 monthly federal supplement guaranteed through July. Alabama is forfeiting millions of federal dollars as a result.
That money would help shore up flagging state revenues for education, health care and other vital services. It also would help people meet basic needs and limit the coronavirus’s spread during an unprecedented economic and health crisis. Forcing people back to workplaces while COVID-19 is still rampant is a dangerous attempt to restore Alabama’s inequitable economic structure.
Alabama should move forward, not return to past failures
The pandemic has shined a light on many of Alabama’s policy mistakes. The state can take this opportunity to fix harsh, shortsighted policies that devalue and harm Alabamians. And our leaders must take the lead on implementing helpful policies because of a lack of comprehensive federal action. The U.S. Department of Labor has issued no guidance allowing workers in high-risk groups to stay home and retain benefits. And the department has not reinforced health and safety protections for workers whose employers don’t take proper coronavirus precautions.
As a result, many older adults, cancer survivors and immunocompromised people face a stark choice between their lives and livelihoods. They must either subject themselves to a higher chance of death from COVID-19 or risk hunger and homelessness when the state cuts off UI benefits. Black and Latino people, women and struggling families will bear the brunt of this callous undermining of the safety net.
Job losses during the COVID-19 economic crash kicked 69,000 Alabamians off their health insurance between February and May, according to a new report by Families USA, a nonprofit research organization based in Washington, D.C.
Those coverage losses increased Alabama’s uninsured rate for non-elderly adults to 19%, the report finds. That is the ninth highest rate in the nation and 3 percentage points higher than in 2018. As workers and their families lose comprehensive health insurance, their risk of delayed care and complications from the virus increases. So does their risk of financial devastation.
“Even before COVID-19, Alabama’s failure to expand Medicaid left more than 220,000 adults uninsured,” Alabama Arise campaign director Jane Adams said. “Further coverage losses during the recession will bring health and financial suffering for even more families across our state. More people will go without needed health care. More hospital bills will go unpaid. And all Alabamians will bear the additional strain on our health care system. This report’s findings should be a blaring emergency siren for our state leaders.”
The number of uninsured adults jumped by 5.4 million nationally between February and May. The increase in those few months was 39% higher than any annual increase ever recorded, Families USA finds. The report also shows a disturbing overlap between states with the highest adult uninsured rates and the worst COVID-19 case trends.
“COVID-19 is putting lives, livelihoods and economic security at risk for thousands of Alabama workers. And many communities face long-term challenges for health care capacity and economic recovery,” Adams said.
“Alabama Arise and Cover Alabama urge Gov. Kay Ivey to save lives and stabilize our local hospitals by expanding Medicaid. We ask the Legislature to provide the needed state share of this pro-family, pro-health, pro-community investment in our future. And we ask Congress to strengthen Medicaid funding and help Alabama shore up our health care infrastructure.”
Adams directs Cover Alabama, a coalition of more than 90 organizations pushing for Medicaid expansion in Alabama. Arise is a founding member of the coalition.
ALABAMA MEDICAID supports the health care system that serves us all. Whether you have employer health coverage, a private plan, public insurance like Medicaid or Medicare, or no coverage at all, you will likely benefit at some point from facilities and services that Medicaid makes possible.
More than a million Alabamians — mostly children in families with low incomes, seniors in long-term care and people with disabilities — have Medicaid coverage that allows them to get the regular, timely medical care they need. By building on this foundation to make affordable coverage more widely available, we can strengthen our health system, our workforce, our communities and our economy.
This report looks at Alabama Medicaid from four angles: how it works now, how it’s improving coverage, who’s still left out and how we can make it stronger.
Click on the icons below to read each section of our report. Please continue below the icons for our conclusion, editor’s note and acknowledgments. You can click any image in this report to enlarge it. To read our news release on the report, click here.
How does Medicaid work in Alabama? (Section 1)How is Medicaid improving coverage? (Section 2)Who’s still left out of health coverage? (Section 3)How can we make Alabama healthier? (Section 4)
Conclusion
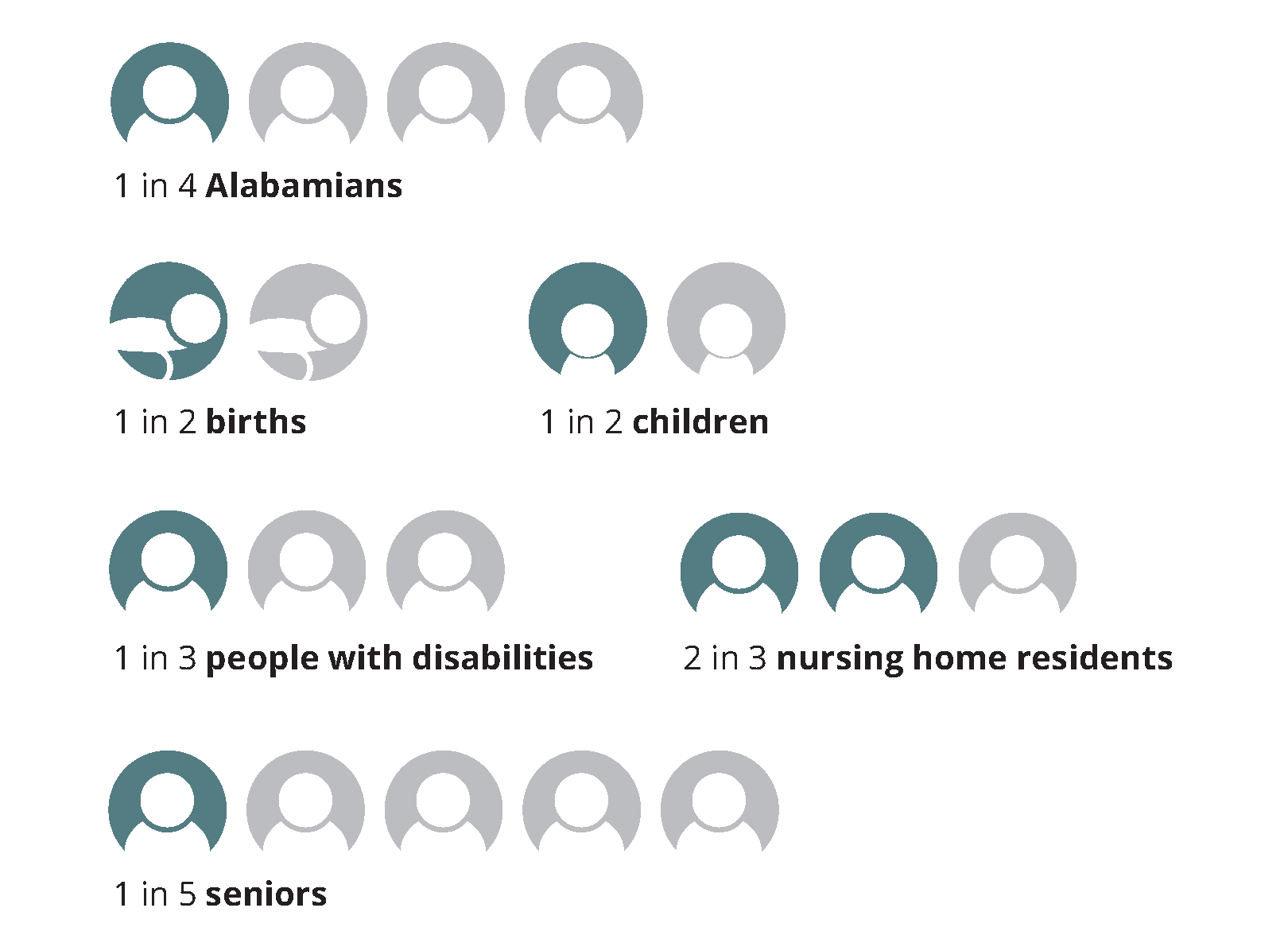
All Alabamians deserve the opportunity to get the health care they need to survive and thrive. Medicaid is a lifeline for one in four Alabamians and an economic engine for communities across our state. Extending Medicaid coverage to adults with low incomes would make life better for Alabamians of all races, genders, hometowns and incomes — and it would only cost the state a dime on the dollar. Here’s why Medicaid expansion is a bargain Alabama can’t afford to pass up:
Medicaid expansion would ensure health coverage for:
People who work low-wage jobs and can’t afford private coverage
Workers who are between jobs
Adults caring for children or other family members at home
People who have disabilities and are awaiting SSI determinations
College students
Uninsured veterans
People harmed by racial and ethnic health disparities
Medicaid expansion would help more Alabamians have:
Regular primary care and preventive checkups
Earlier detection and treatment of serious health problems
Regular OB/GYN visits without referral
Less dependence on costly emergency care
Better health and greater financial peace of mind
Medicaid expansion would bring our federal tax dollars home to support:
Better outcomes on critical health challenges like infant mortality, obesity and substance use disorders
Stronger rural hospitals and clinics
A stronger network of community mental health and substance use disorder services
A needed boost in jobs and revenue for state and local economies
Editor’s note
As we publish this report, Alabama and the world are facing the public health emergency of the COVID-19 pandemic. The duration and fallout of the crisis are impossible to predict, but every level of our health care system will be severely tested in the months ahead. The pandemic is taking a disproportionate toll on African American and Latino communities where people are more likely to live in poverty and without health insurance. And the number of uninsured Alabamians — already shockingly high before the pandemic — will continue to grow as unemployment mounts.
In times like these, state leaders play a crucial role in protecting the public from physical, mental and financial harm. One of the most important tools available to both elected officials and their constituents is accurate information about how state services promote the common good — and how we can make them stronger.
While this report took shape before the COVID-19 crisis erupted, we hope it will help Alabamians understand the available health care solutions and their important economic benefits. Emergencies demand rapid response, and an understanding of the “preexisting conditions” in our state’s health care system can make those responses more appropriate and more effective.
Through this pandemic and the next one — and the more ordinary times in between — all Alabamians will depend on a health care system with Alabama Medicaid at its core. The stronger Medicaid is, the better the prognosis for all of us will be.
The COVID-19 emergency has brought several temporary changes to the information in this report, including the following:
Section 1
Silvia Hernandez has suspended services at Go Play Therapy but hopes to reopen after the economy stabilizes.
Section 1
Congress has increased the federal share of Medicaid funding for all states by 6.2 percentage points for the length of the pandemic. Some lawmakers have proposed further increases.
Section 2
If someone had Medicaid coverage during March 2020, Alabama will not end that coverage during the pandemic unless the person cancels it or moves out of state. This temporary halt to coverage cuts includes people receiving postpartum coverage that normally ends after 60 days.
Acknowledgments
This Alabama Arise report was made possible by a generous grant from The Women’s Fund of Greater Birmingham. The findings and conclusions presented in this report are those of Arise and do not necessarily reflect the opinions of The Women’s Fund.
Arise policy director Jim Carnes was the primary author of this report, and Valerie Downes of Montgomery designed it. Arise communications associate Matt Okarmus interviewed many of the individuals profiled in this report. Other report editors and contributors included Arise executive director Robyn Hyden; communications director Chris Sanders; policy analyst Carol Gundlach; organizing director Presdelane Harris; organizers Stan Johnson, Mike Nicholson and Debbie Smith; and intern Kayla Thompson.
Special thanks to Jesse Cross-Call and Tammie Smith at the Center on Budget and Policy Priorities and Stephen Eisele and Paul Gels at Community Catalyst for their guidance and support.
Medicaid is a joint federal/state program providing health coverage for certain categories of people with low incomes and limited resources.
More than 1.2 million Alabamians qualify for Medicaid coverage.
Medicaid payments support doctors’ offices, hospitals, clinics and nursing homes that serve all Alabamians.
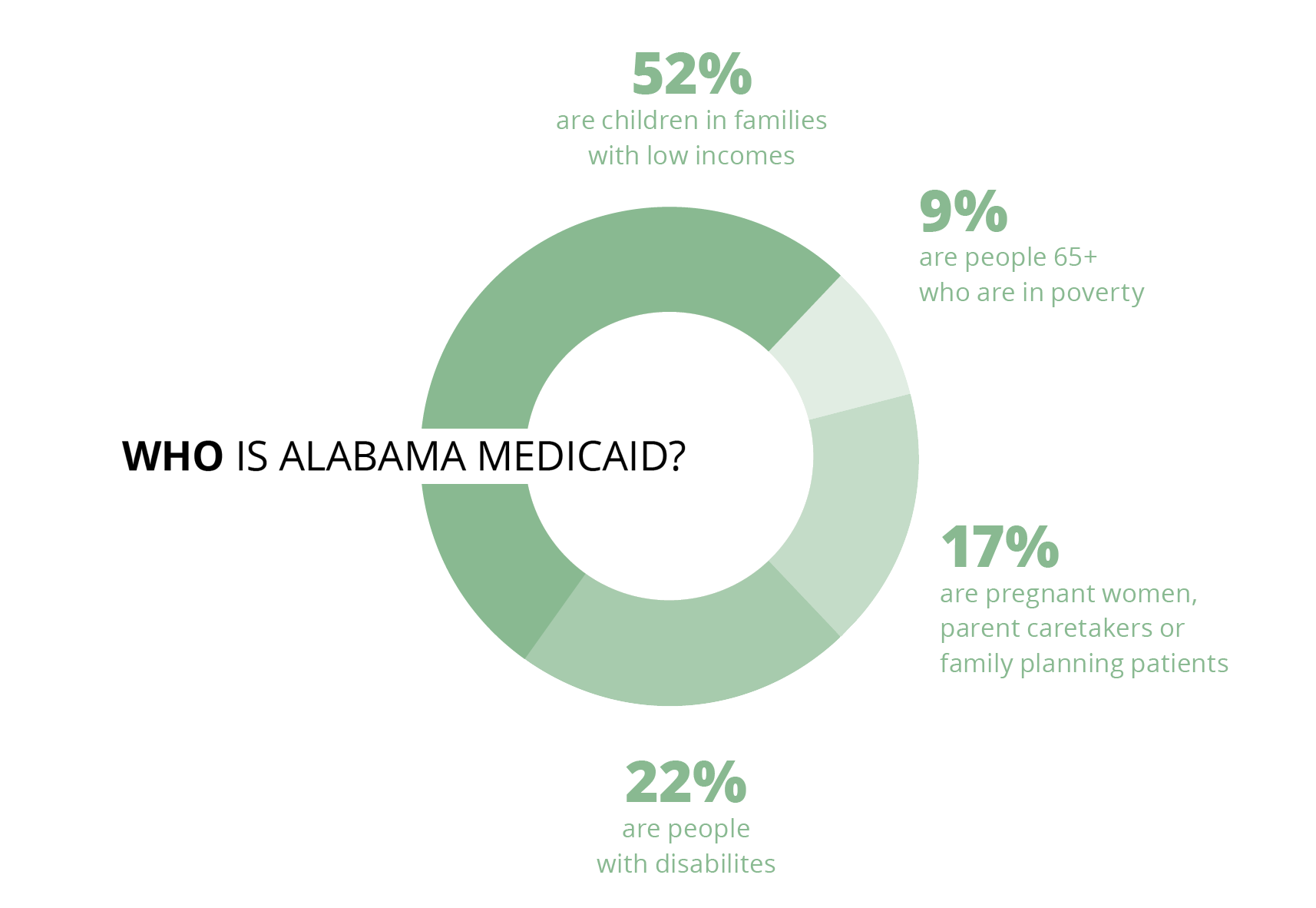
Children make up more than half of Alabama Medicaid beneficiaries.
Medicaid also provides essential coverage for seniors, pregnant women, and people with disabilities.
Alabama Medicaid’s eligibility limits are among the nation’s most restrictive.
Medicaid is the backbone of our health care system
More than 1.2 million Alabamians, or 25% of our state’s population, qualified for Medicaid coverage in fiscal year 2017. Looking closer, that’s:
Medicaid pumps $7 billion in federal and state money into our health care system every year. Without Medicaid funding, many of the doctors’ offices, clinics, hospitals and other medical facilities that all Alabamians depend on would have to cut services or close.
SPOTLIGHT
Meet Silvia Hernandez
Silvia Hernandez of Fort Payne opened Go Play Therapy after her son’s speech challenges revealed a shortage of therapists in her area. (Photo: Matt Okarmus)
To get her son the speech therapy he needed a few years ago, Silvia Hernandez of Fort Payne had to drive him two hours each way to the recommended therapist in Birmingham. Her top priority was her son’s health care, but Silvia saw firsthand the hurdles of time and resources that some parents in her area would have trouble getting over.
When Silvia encounters a problem, she goes to work — this time literally. Today, she is the owner of Go Play Therapy, a practice she built and opened in response to the provider shortage in her area. Go Play specializes in occupational, physical and speech therapy for children up to age 18. There are two Go Play locations, in Fort Payne and Centre.
Hernandez estimates 90% of her clients have Medicaid.
“If Medicaid didn’t exist, we’d have to shut our doors,” Silvia says. She adds that extending Medicaid coverage to adults with low incomes — not just their children — would help even more people gain access to the care they need. As a business owner, she sees another advantage to Medicaid expansion: It would allow her to expand her therapy office and hire additional employees.
Who is Alabama Medicaid?
Source: Alabama Medicaid
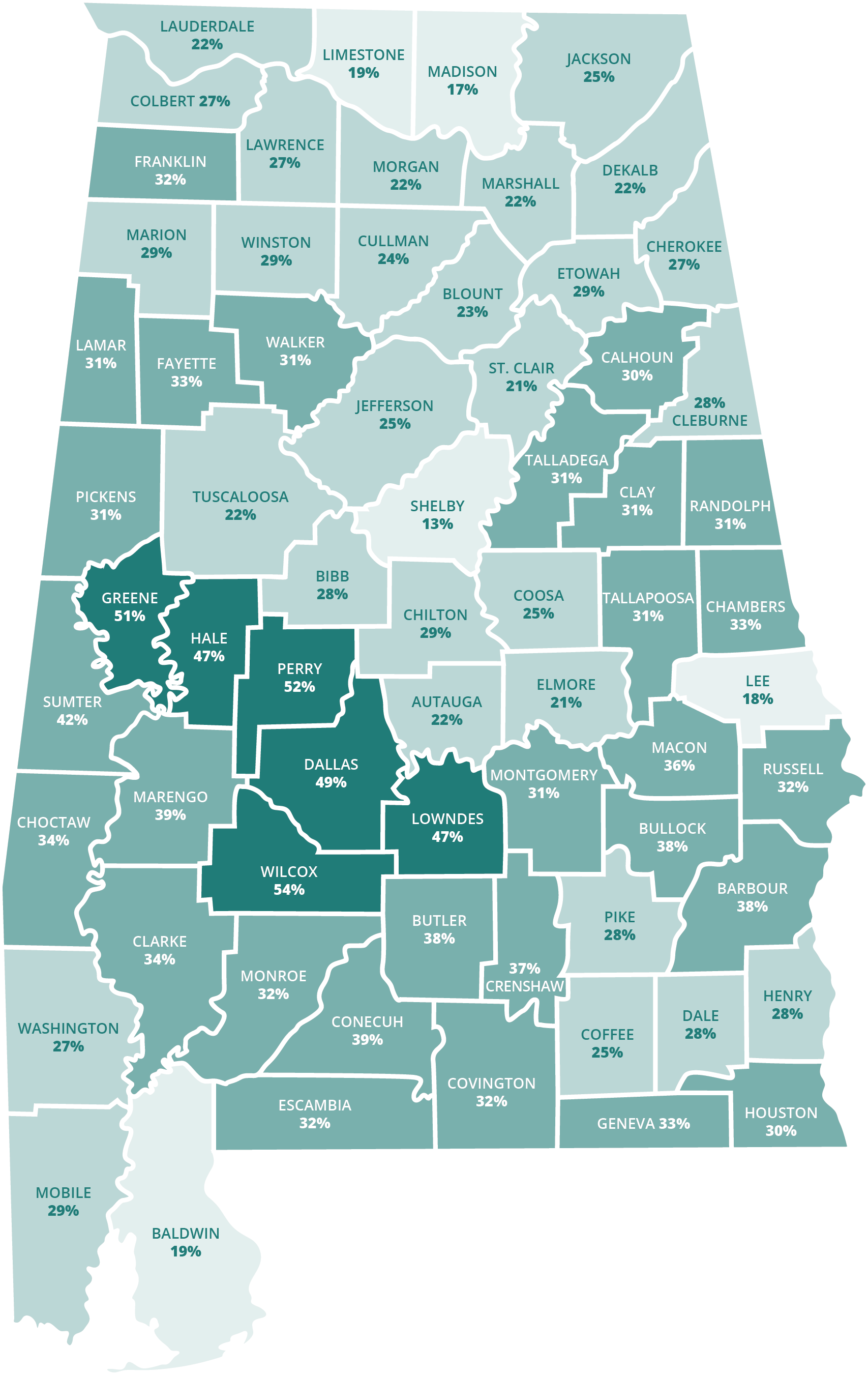
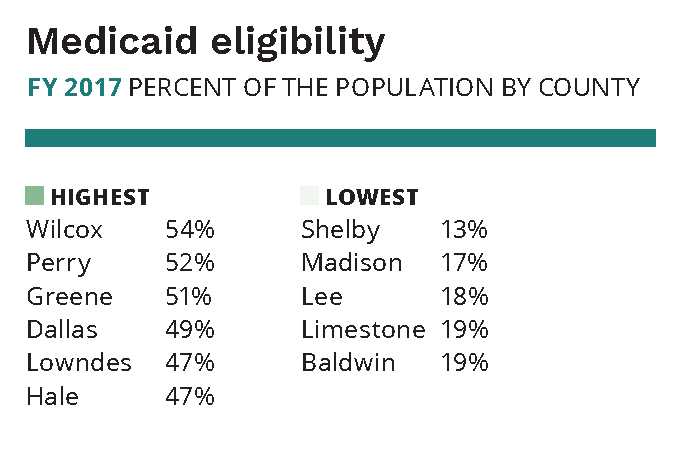
Alabamians in every county qualify for Medicaid
About one in every six Alabamians lives in poverty. For children, the rate is nearly one in four. Even Alabama’s most prosperous counties have significant numbers of households living below or near the poverty level. That means Medicaid is a lifeline for families across the entire state.
Source: Alabama MedicaidSource: Alabama Medicaid
How do people qualify for Medicaid coverage in Alabama?
When an individual or family applies for Medicaid, a number of factors determine whether they’re eligible and which program would best serve their needs. Age, income, family size and certain health conditions like pregnancy or disability all play a part.
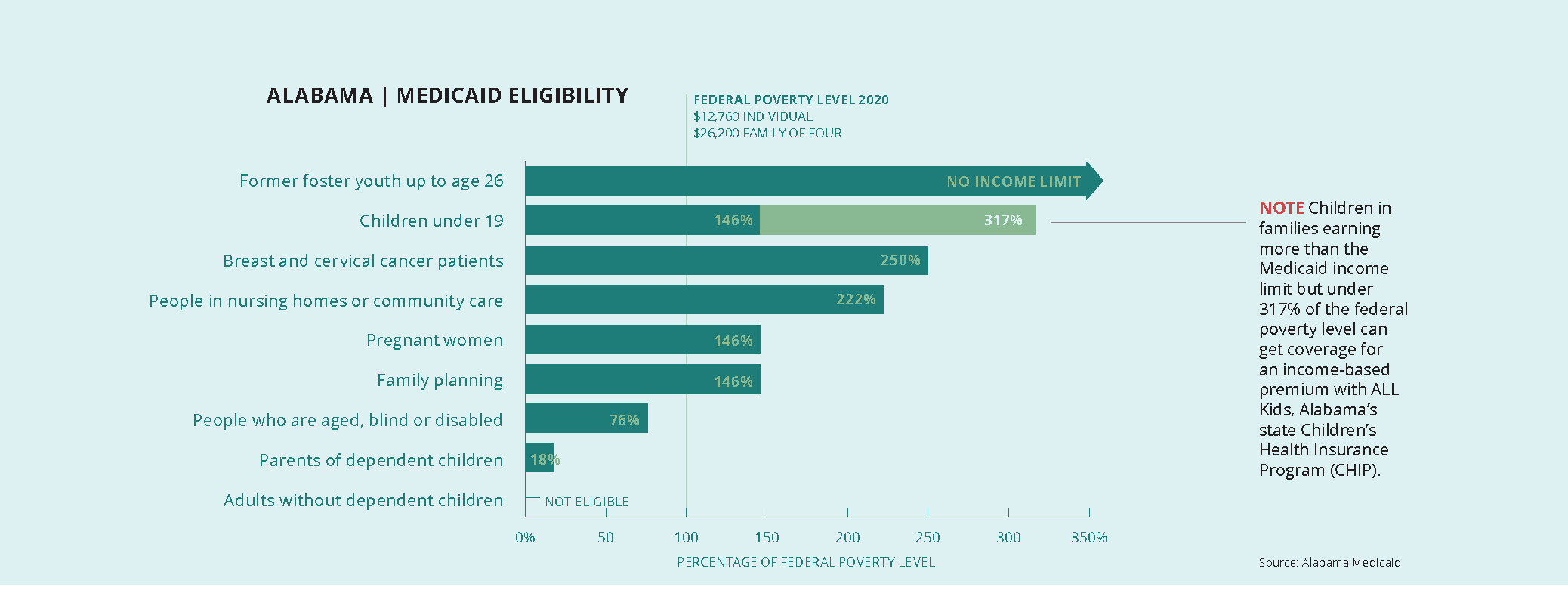
The household income limit for a particular program is expressed as a percentage of the federal poverty level (FPL) — often in shortened form, such as “146% of poverty.” The higher the percentage, the more income an individual or family may have and still qualify for Medicaid.
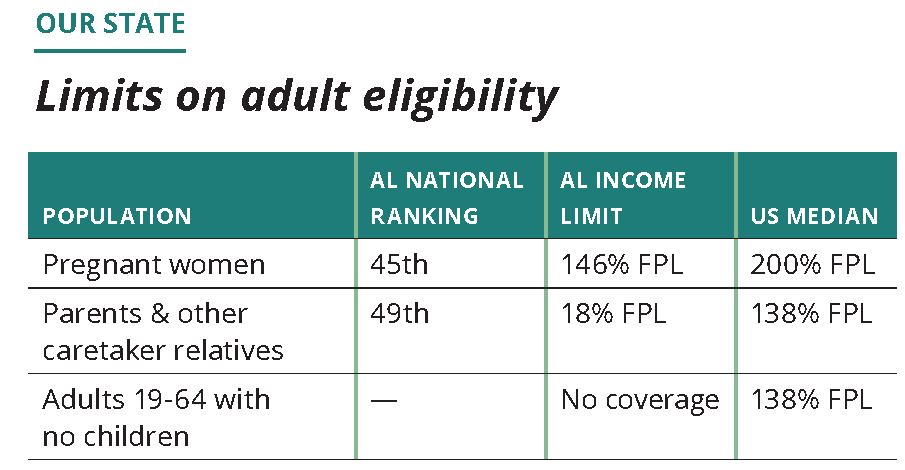
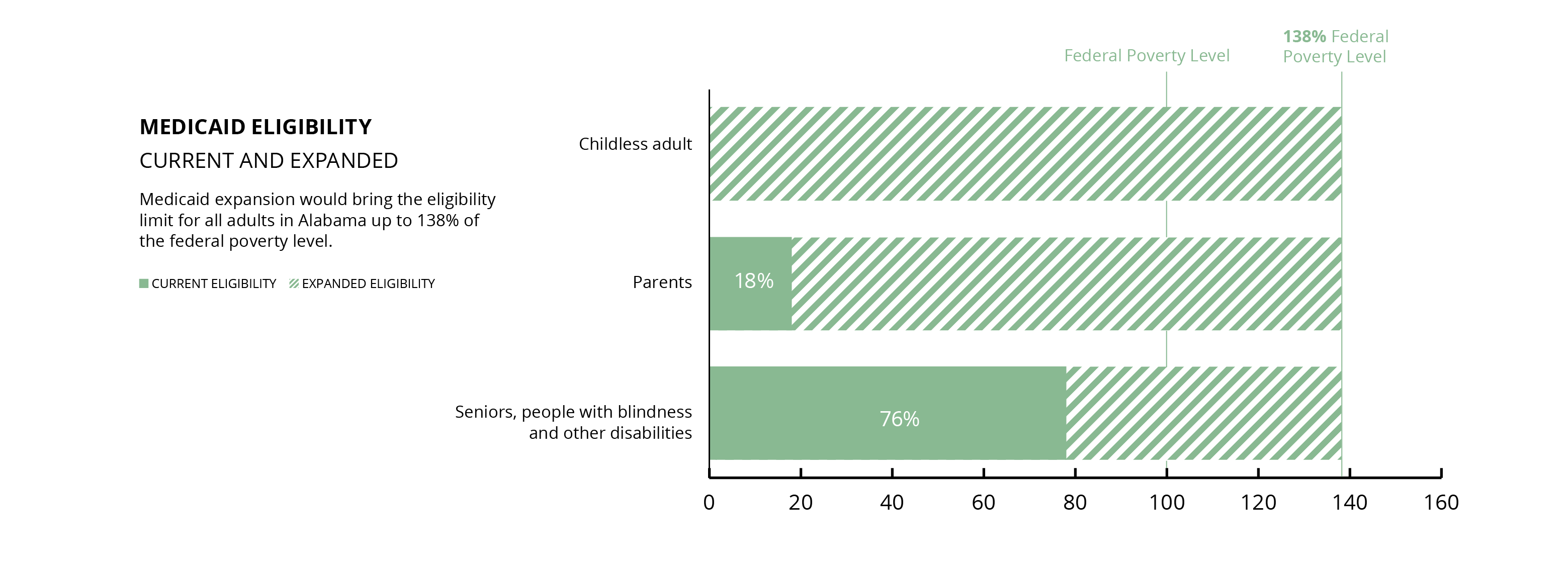
The income limits for Alabama Medicaid’s eligibility groups are shown below. In 2020, the FPL was $12,760 for an individual and $26,200 for a family of four.
How does Alabama’s Medicaid eligibility compare?
Children’s health coverage has long been a point of pride for Alabama. We were the first state to launch a Children’s Health Insurance Program (CHIP) after Congress created that option in 1997. While our family income limit for children in Medicaid is the third lowest in the country at 146% FPL, ALL Kids covers children above the Medicaid limit up to 317% FPL. That puts Alabama among the top 10 states for CHIP eligibility. For working-age adults, however, Alabama Medicaid’s income limits tell another, far more troubling story.
National ranking: 49th
For adults without children or a disability, we’re one of 14 states that offer no Medicaid coverage. And only Texas makes it harder than Alabama for parents of dependent children to get Medicaid coverage.
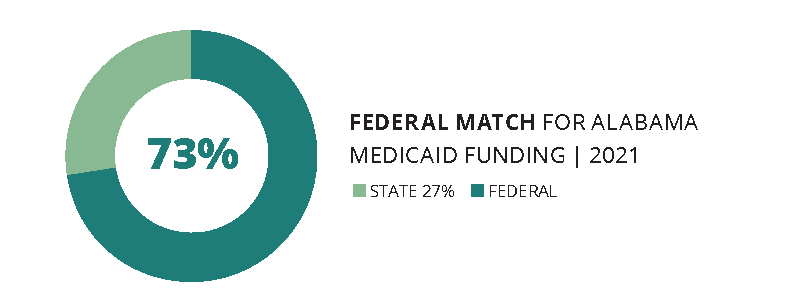
How does Medicaid funding work?
The federal government pays at least half of each state’s Medicaid costs. The percentage (called the Federal Medical Assistance Percentage, or FMAP) is set annually through a complicated formula based on per capita (or per person) income. The lower the state’s per capita income, the higher the FMAP, up to a maximum 83%. Alabama’s FMAP for FY 2021 will be 72.58%. This means we get roughly $7 in federal money for every $3 Alabama pays for Medicaid. Alabama Medicaid’s total annual budget is about $7 billion.
State money for Medicaid comes from a number of sources, including the General Fund (GF), special trust funds, and transfer payments from public hospitals. Because the revenues earmarked for the GF come from minor taxes, fees and interest payments that grow slowly, Medicaid and other GF services remain permanently shortchanged.
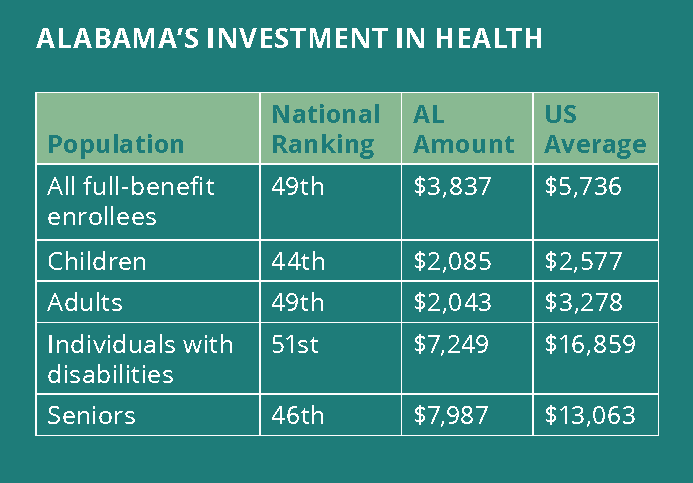
How does Alabama’s Medicaid investment compare?
One simple way to compare Medicaid programs across states (and the District of Columbia) is to rank their spending per enrollee in major Medicaid eligibility groups. Spending is only one factor in the delivery of care, but it does indicate the investment that the state is willing to make in the health of residents with low incomes. Here’s how Alabama measures up on that count:
Source: Kaiser Family Foundation, State Health Facts 2014
What services does Medicaid cover?
To qualify for federal funding, state Medicaid programs must cover:
Well-child check-ups, known as EPSDT (Early Periodic Screening, Diagnosis and Treatment, including dental services), for all Medicaid-eligible children under age 21. Because most Medicaid beneficiaries (also known as members) are children, EPSDT is the most wide-reaching Medicaid service.
Inpatient and outpatient hospital care.
Doctor services.
Laboratory and X-ray services.
Skilled nursing.
Family planning services.
Pregnancy-related services.
Ambulance services.
Alabama is one of only three states where Medicaid does not cover any dental care for adults.
The federal government also identifies optional Medicaid services that states may offer. Alabama offers only a few of these, including adult prescription drug coverage, adult prosthetics and community-based hospice care. In addition, Alabama has waivers, or special permission, to offer home- and community-based long-term care and regionally based coordinated primary care.
IN FOCUS
Children with special health care needs
Alabama Medicaid and ALL Kids together cover more than 105,000 children with special health care needs. These children are at increased risk for chronic physical, developmental, behavioral or emotional conditions. They require services tailored to these needs.
The Medicaid portion of this population includes more than 21,000 children who received Supplemental Security Income (SSI) in 2018. A child receiving SSI has a medically determinable physical or mental impairment, including emotional or learning problems, that results in marked and severe functional limitations and has lasted or can be expected to last for a continuous period of at least 12 months.
A SENSE OF SCALE: 105,000 children are more than the capacity of Bryant-Denny Stadium (101,821). (Photo: AP Images)
SPOTLIGHT
Meet Mattisa Moorer and Kerstin Sanders
Kerstin Sanders and her mom, Mattisa Moorer, have become champions for special education services in Lowndes County schools. (Photo: Judy Barranco)
Like many teenagers, Kerstin Sanders enjoys movies, being out in the crowd, chilling out and sleeping in. Cerebral palsy, Dandy Walker Syndrome, epilepsy, scoliosis and restrictive lung disease are facts of her life, but they aren’t her life.
Kerstin is a treasure to anyone who takes the time and effort to know her, says her mother, Mattisa Moorer.
As Kerstin ages, her care becomes more complex. For example, multiple surgeries and procedures have made it necessary to change her feeding tube more frequently. Medicaid pays for most of the medications and supplies that Kerstin needs every month.
“It’s been a life-saver,” Mattisa says.
The Lowndes County single mom realized she would need to be an advocate for her daughter when Kerstin entered Head Start. At first, the school’s special education coordinator listened carefully and designed a plan that allowed Mattisa to be a classroom aide. But a change of administration caused the plan to unravel.
“I saw that I need to continuously advocate for Kerstin’s inclusion and, at middle school, her access,” Mattisa says. That calling now has expanded to include working part-time as a parent consultant with Family Voices of Alabama and serving as a consumer representative with her local Alabama Coordinated Health Network (ACHN).
While patient advocacy has come with struggles — waiting lists, paperwork, hard-to-obtain information — Mattisa values her successes. She considers the camaraderie of others in similar situations to be one of her biggest wins.
Medicaid Matters (Main Section)How is Medicaid improving coverage? (Section 2)Who’s still left out of health coverage? (Section 3)How can we make Alabama healthier? (Section 4)
New Medicaid changes seek to improve health and cut costs by rewarding timely and preventive care.
The statewide Integrated Care Network (ICN) is coordinating long-term care for about 23,000 Alabamians.
Seven regional Alabama Coordinated Health Networks (ACHNs) are coordinating primary and specialty care for about 750,000 Alabamians.
The ICN and ACHNs have Consumer Advisory Committees and consumer representatives on their boards.
ACHNs have identified infant mortality, obesity and substance use disorders as top priorities for improvement.
Steps in the right direction
Recent changes in the way Medicaid members get their care are promising moves in the right direction. By rewarding prevention and appropriate, timely care, Medicaid hopes to improve health outcomes, while bringing costs down in the process.
The new plans can be a significant improvement over the old Medicaid system, if they keep the focus on better health. One way to improve the chances for success is to have a strong consumer voice at the policy table. The changes are happening on two tracks:
Long-term care for people who need assistance with activities of daily living.
Primary care for children and pregnant mothers.
Public policy is better and more responsive when people have a say in decisions that affect their health and well-being. And Alabama Medicaid reforms are lifting those voices.
Rethinking Medicaid long-term care
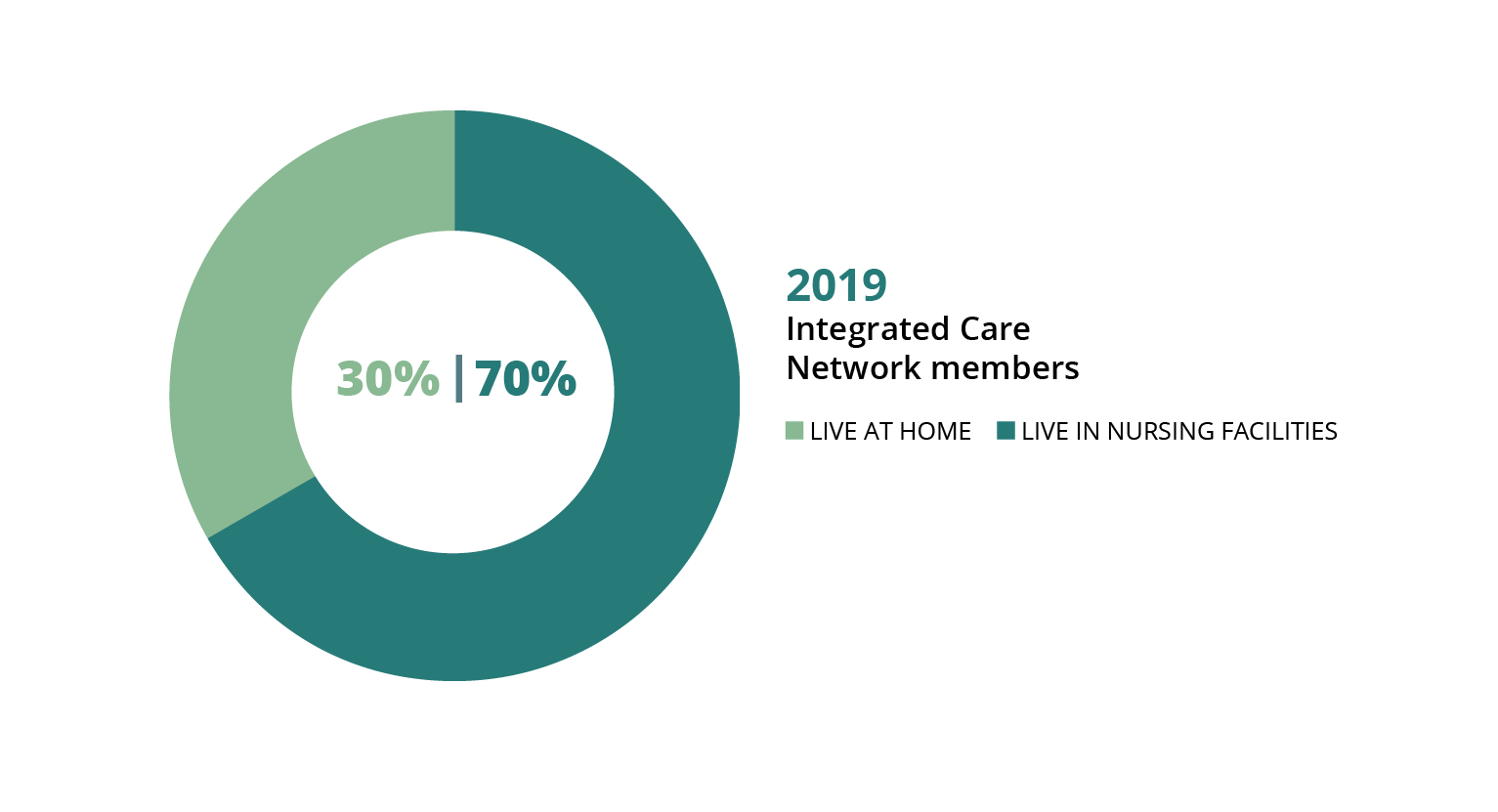
For long-term care patients, Medicaid has a new plan called the Integrated Care Network (ICN). The ICN coordinates care for Medicaid members who live in nursing facilities or receive certain home- and community-based waiver services. There are only about 23,000 of these members across Alabama, so one statewide ICN serves all of them.
In 2019, roughly two-thirds of people served by the ICN lived in nursing facilities, and about one-third were living at home. The goal of the program is to help more people get long-term care services in their home and community, if that’s what they want. The ICN works with the 13 Area Agencies on Aging across the state to coordinate long-term care for Medicaid members who qualify.
The ICN also has a strong consumer voice at the policy table. Four consumer advocates serve on the governing board. And the Consumer Advisory Committee (CAC) includes eight consumer representatives. The chairperson of the CAC (Dr. Eric Peebles, featured below) receives home-based long-term care services through a Medicaid waiver.
AREA AGENCIES ON AGING: Thirteen Area Agencies on Aging (plus the Regional Planning Commission of Greater Birmingham) provide care coordination for ICN members. Visit the ICN website at alabamaselect.com to learn more about the regional organizations. (Source: Alabama Department of Senior Services)
SPOTLIGHT
Meet Dr. Eric Peebles
For Dr. Eric Peebles of Auburn, the path of advocacy for independent living began in an upstate New York elementary school. (Photo: Matt Okarmus)
School officials in the New York community where Eric Peebles grew up tried every excuse in the book to prevent him from starting school. “We can’t find him an appropriate classroom aide,” they said. Or “his power wheelchair is a danger to the other students.”
It was the mid-1980s, and federally mandated special education was still a relatively new policy. But those officials didn’t know what they were getting into when they threw roadblocks in the path of Eric and his mom, Pat. Two years, multiple runarounds and a lawsuit later, Eric’s school district found itself under federal supervision, and all district administrators involved in his case lost their jobs. His mother was appointed to the search committee for their replacements.
Thanks to his mom, Eric got an early education in self-advocacy. That groundwork served him well 25 years later when he moved to Alabama to complete his doctorate and join the undergraduate faculty in rehabilitation and disability studies at Auburn University. His personal experience with spastic cerebral palsy (resulting from oxygen deprivation at birth) gives him an insider’s perspective on disability policy and services — and on stereotypes. One misconception he fights hard to dispel is the assumption that his advocacy is aimed solely at asserting his own rights and opportunities, rather than those of all people with disabilities.
‘Greater things to come’
When Eric moved here nearly 10 years ago, Alabama Medicaid’s long-term care services were so sparse that he maintained his residency in another state until the menu of services expanded. Today, he enjoys community self-sufficiency through his participation in the Alabama Community Transition (ACT) waiver. In addition to running his own research and consulting business, Accessible Alabama, Eric serves on the board of the Disabilities Leadership Coalition of Alabama and chairs the Medicaid Integrated Care Network (ICN) Consumer Advisory Committee. In 2019, Gov. Kay Ivey appointed him to the State of Alabama Independent Living Council.
Those long-ago school officials left a mark they couldn’t foresee. Among all his achievements, Eric counts the success of his own former students as a special point of pride. But his advocacy story is still being written, he says. “It feels like these accomplishments are forerunners of greater things to come.”
A regional approach to Medicaid primary care
Under Alabama Medicaid’s new structure, seven regional Alabama Coordinated Health Networks (ACHNs) coordinate primary care for Medicaid children, pregnant mothers and people who receive family planning services. Primary care includes well-child visits; EPSDT (Early Periodic Screening, Diagnosis and Treatment) for children; adult screening, diagnosis and treatment; and preventive care.
Each member can choose a primary care doctor to be their “patient-centered medical home.” Each ACHN has a phone line to call when a Medicaid participant has a health problem. The basic idea is that nurses, social workers and care coordinators working with the primary care doctor can help people get the right care for the right problem without going to the emergency room whenever they get sick.
Seven regional networks provide primary care coordination for ACHN members. Visit medicaid.alabama.gov to learn more about the ACHNs.
Medicaid ACHNs bring a new focus on consumer engagement and better health
The regional network plan gives Medicaid new tools for improving health outcomes. The ACHN can help patients identify health goals, create a care plan and connect with community resources that promote better health. The new plan serves about 750,000 Medicaid members across seven regions. Each ACHN has a consumer representative on its board, in addition to a Consumer Advisory Committee (CAC).
Bonus payments for doctors who reach quality benchmarks are another feature aimed at improving care. Each ACHN also is conducting Quality Improvement Projects (QIPs) targeting three health measures for improvement:
Infant mortality
Obesity
Substance use disorders
Medicaid consumer representatives in Alabama have teamed up for training and peer support. (Photo: Renée Markus Hodin)
SPOTLIGHT
Meet Audrey Trippe
Navigating the complicated system of mental health and substance use services motivated Audrey Trippe of Attalla to step up and serve as a Medicaid consumer representative. (Photo: Courtesy of Audrey Trippe)
Audrey Trippe, a resident of Attalla in Etowah County, has worked in mental health care since 2013, serving as a peer support specialist, peer supervisor, youth peer and certified addiction counselor. She and her husband are the proud parents of two boys, one of them a newborn.
Audrey considers herself in long-term recovery from major depression and substance use disorder. She has spent most of her young adulthood in the coverage gap, relying on urgent care clinics and the ER. Being heard has been a challenge.
“There have been times I’ve felt like a chart and not a person,” she says. “I’ve felt overmedicated at times because I couldn’t communicate what feelings were from my mental issues and what feelings were normal for substance use recovery.”
For a while, Audrey and her husband had enough income to purchase Marketplace insurance, which covered her first pregnancy. But a series of financial setbacks put her back in the gap — and her baby into Medicaid coverage. She qualified for Medicaid herself with her second pregnancy. Now that the baby is born, Audrey’s coverage will expire 60 days after delivery.
‘Great hope for the future’
Navigating these ins and outs, ups and downs has motivated Audrey to help others find their way. That’s why she said yes when a friend at the Alabama Disabilities Advocacy Program asked her to be a consumer representative for her local Alabama Coordinated Health Network (ACHN). She wants to be an “authentic voice” for consumers.
“I want to educate individuals about the options they have and teach them how to have helpful conversations with their own care providers,” she says.
While Audrey faces returning to the coverage gap when her pregnancy coverage expires, she maintains a positive outlook.
“I believe things are getting better all around, and I have great hope for the future,” she says. “There are still things that need to change, but change — like recovery — takes time.”
Priority for improvement
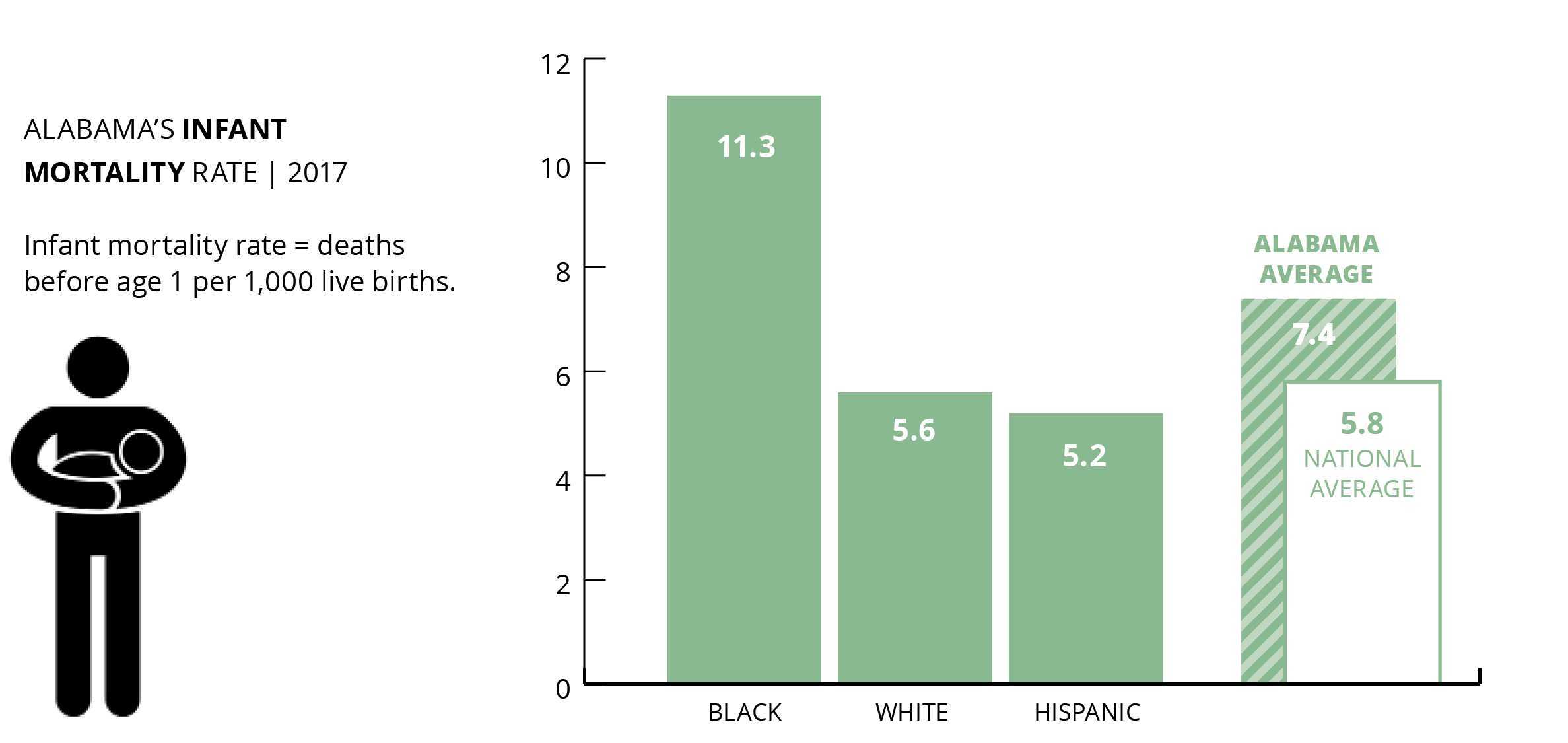
Infant mortality
Alabama’s regional Medicaid networks have identified infant mortality as a key target for improving health outcomes. That’s a promising step. Evidence from Medicaid expansion states shows that providing women continuous health coverage — not just during pregnancy — would make a life-saving difference. Lowering the high rate of African American infant deaths is the key to overall improvement.
National ranking: 45th
Source: VOICES for Alabama’s Children, 2019 Kids Count Data Book
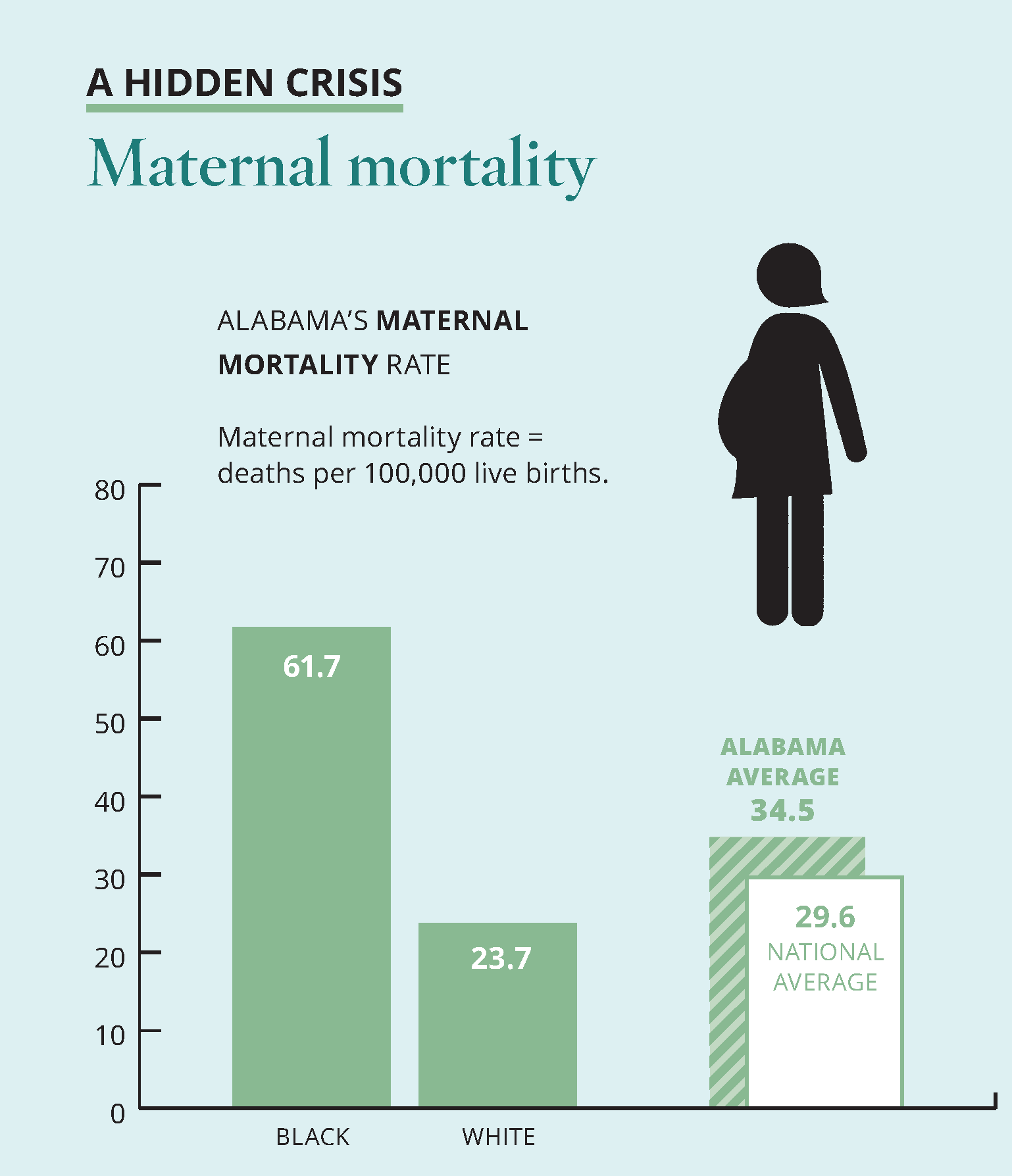
A hidden crisis: Maternal mortality
In late 2019, the Alabama Department of Public Health (ADPH) announced the infant mortality rate for 2018 at a record low 7.0 per 1,000 live births. National comparisons are not yet available. Alabama’s infant mortality rate is improving but remains one of the highest in the country, and racial disparity in birth outcomes is widening.
A particular concern is the continuing increase in the percentage of births with no prenatal care, which rose to 2.4% in 2018, ADPH reports.
Source: America’s Health Rankings, 2019 Health of Women and Children Report
The chief medical causes of infant death include congenital abnormalities, low birth weight and preterm births, Sudden Infant Death Syndrome (SIDS) and bacterial sepsis, according to ADPH. Health researchers are discovering how social factors like place of residence, environmental influences and available resources play a role in determining different outcomes for different racial groups.
Maternal deaths in childbirth occur more rarely than infant deaths, but they are a stark indicator of racial disparities in health care. Black mothers in Alabama die in childbirth at nearly three times the rate of white mothers, and nearly double the overall statewide rate.
Priority for improvement
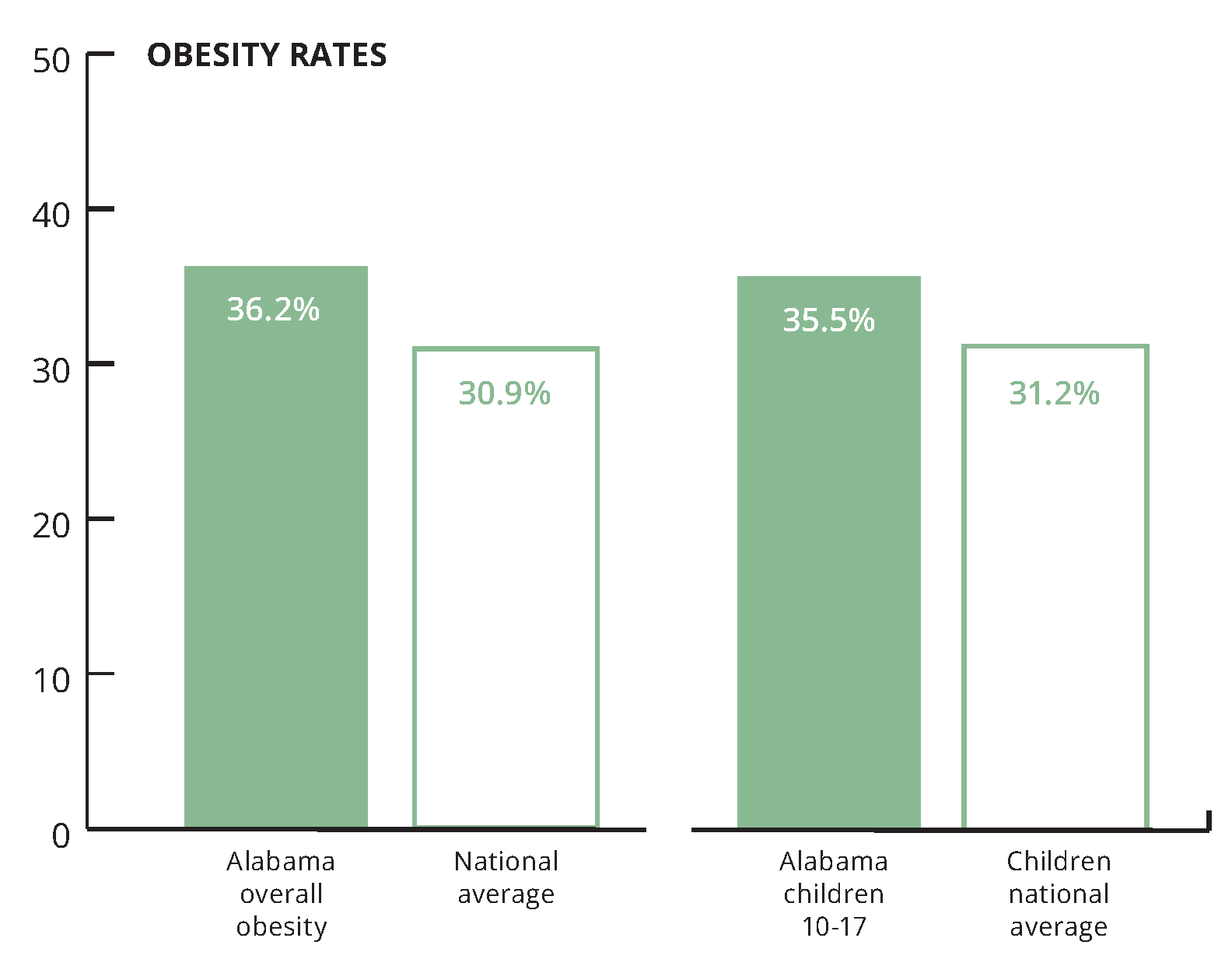
Obesity
Alabama’s regional Medicaid networks are working to reduce the state’s obesity rate. Extending Medicaid coverage to adults with low incomes would allow thousands more Alabamians to benefit. That would mean healthier families and a healthier workforce.
National ranking: 45th
Source: America’s Health Rankings, 2019 Annual Report
A leading cause of obesity is food insecurity, or the inability to provide adequate food for one or more household members because of lack of resources. Families experiencing food insecurity may rely on low-cost, high-energy foods and beverages, which can lead to overconsumption of calories and result in obesity.
16.3% of Alabama households experienced food insecurity in 2019, for a national ranking of 46th. The national average was 12.3%.
Healthy foods, such as fresh fruits and vegetables, are more expensive and less available in some communities than in others. A CDC study found that only 6.1% of Alabama adults meet the daily vegetable intake recommendation. And only 8.8% of Alabama adults meet the daily fruit intake recommendation. Medicaid programs in other states are exploring ways to make healthy foods more accessible and affordable where people live, work, learn and play. (Source: America’s Health Rankings, 2019 Health of Women and Children Report)
Priority for improvement
Substance use disorders
Alabama’s regional Medicaid networks seek to boost the availability of treatment for
substance use disorders. In the past five years, drug deaths in Alabama increased 37%, from 11.7 to 16.1 deaths per 100,000 people. Despite the increase, Alabama’s drug death rate remained below the national average of 19.2 deaths per 100,000. (Source: America’s Health Rankings, 2019 Annual Report)
Medicaid Matters (Main Section)How does Medicaid work in Alabama? (Section 1)Who’s still left out of health coverage? (Section 3)How can we make Alabama healthier? (Section 4)
More than 220,000 Alabamians are caught in the state’s health coverage gap, earning too much to qualify for Medicaid and too little to afford private insurance.
Another 120,000 Alabamians are stretching to pay for coverage they can’t afford.
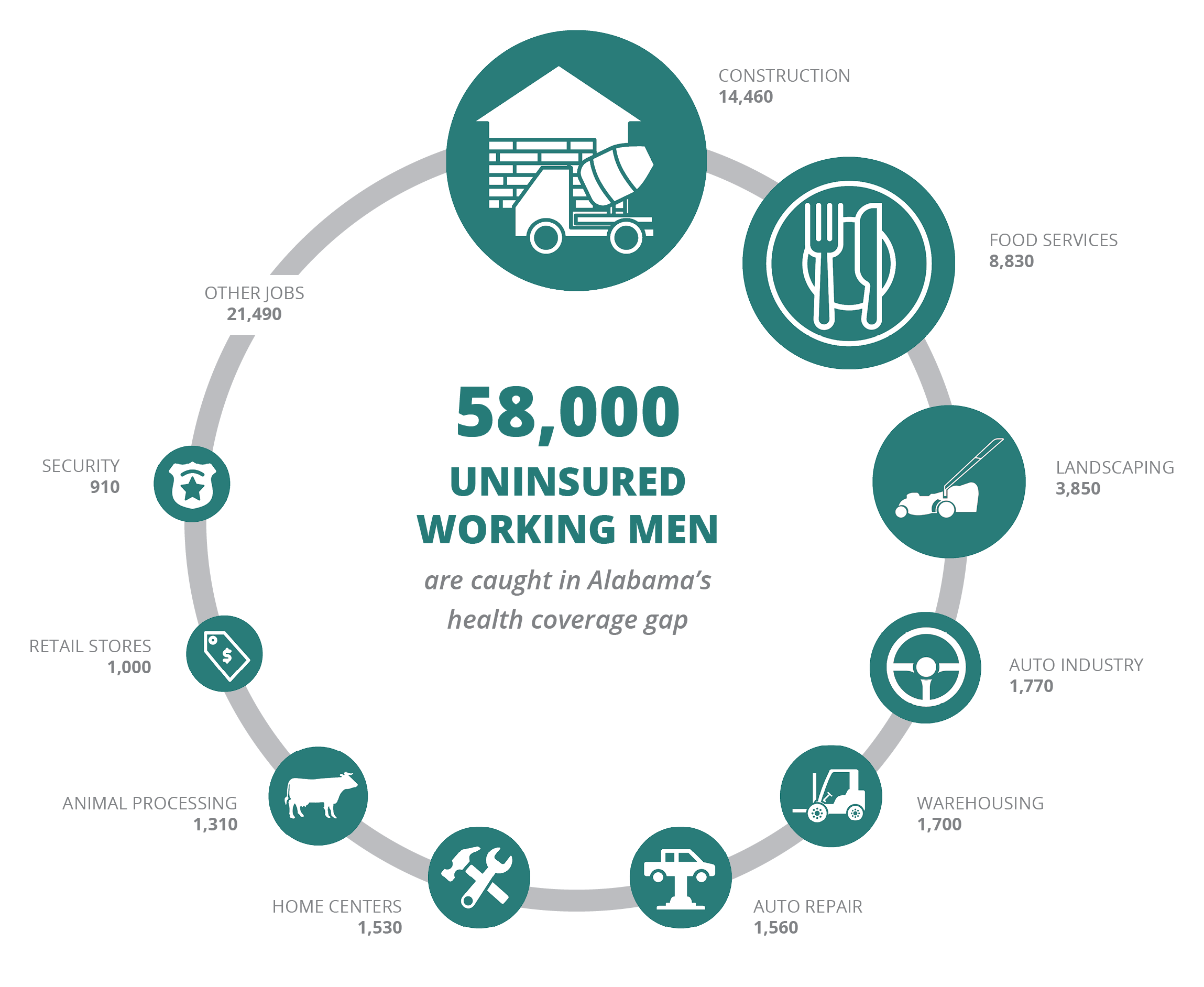
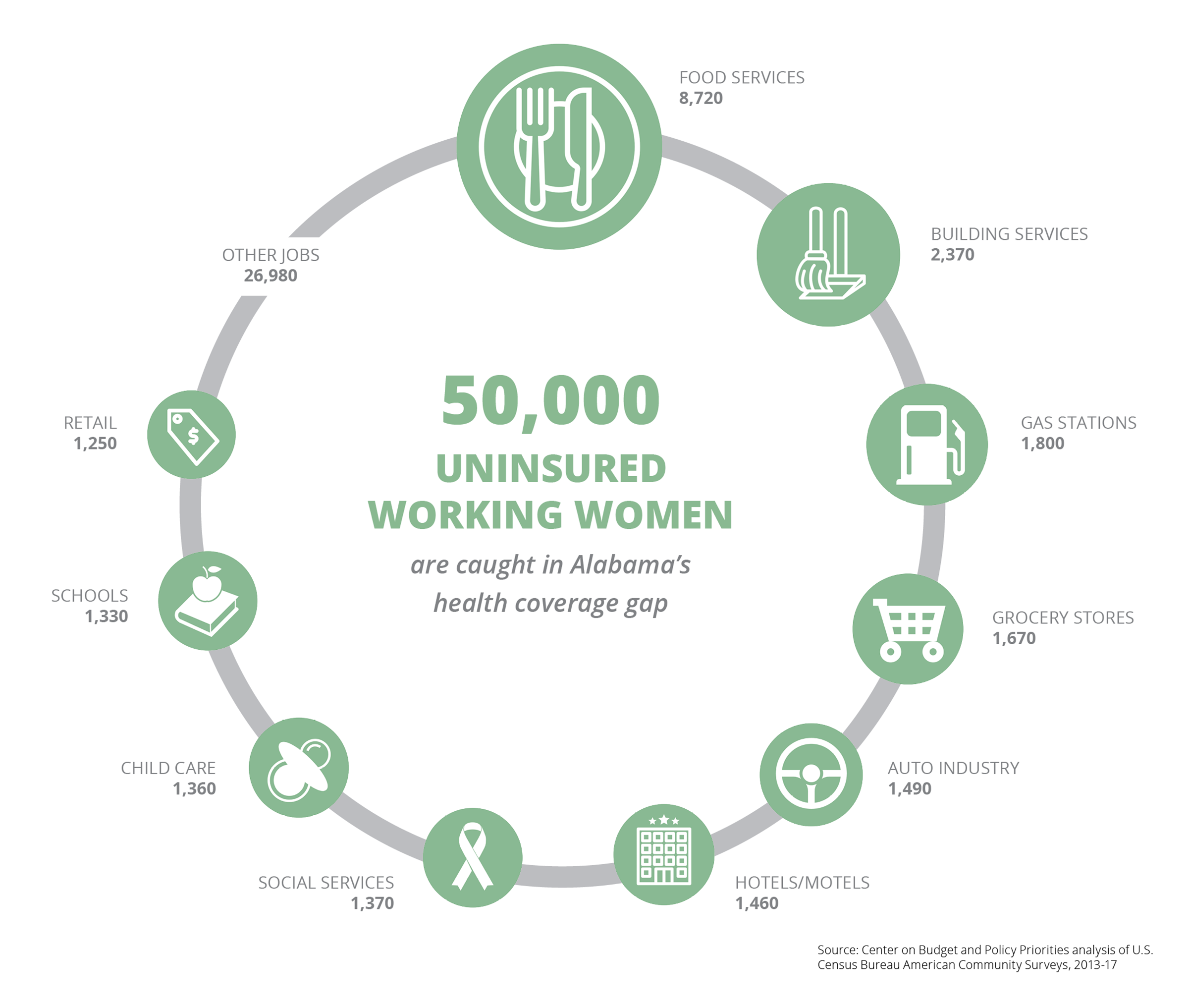
Tens of thousands of Alabamians in the coverage gap are between jobs or are working in essential, low-paying fields like child care, construction and food service.
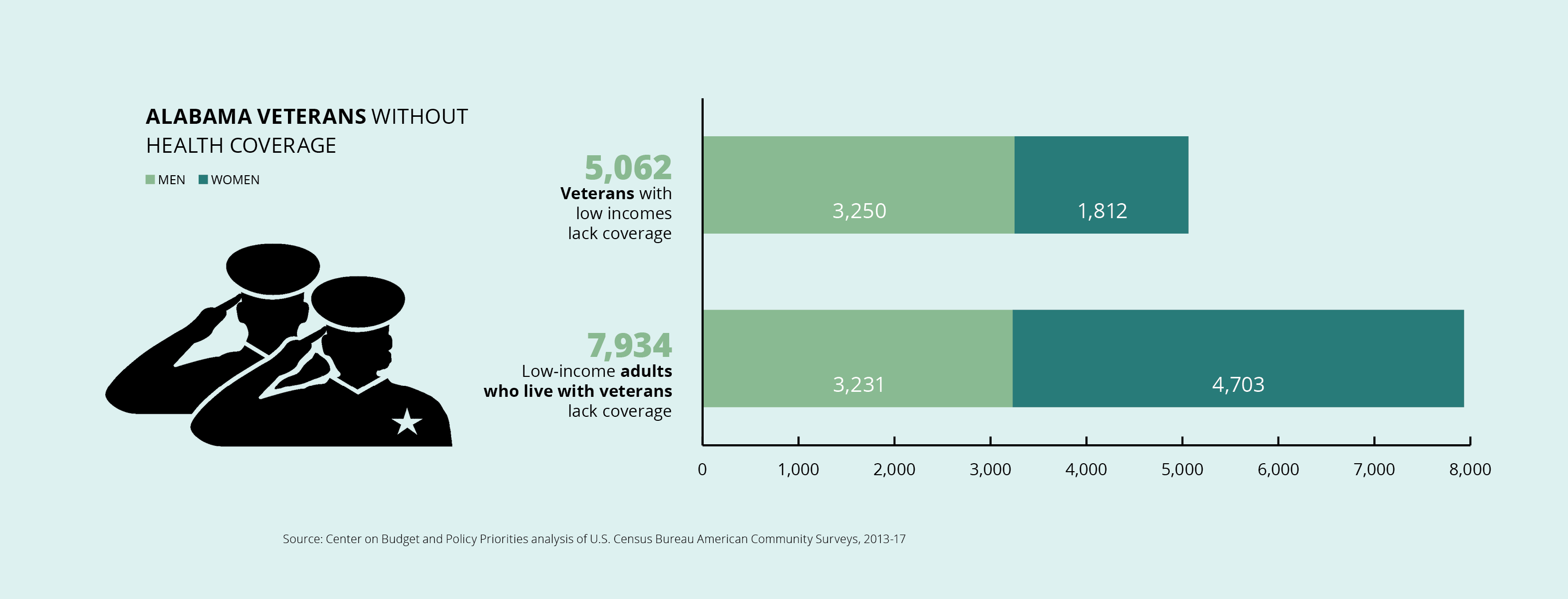
13,000 Alabama veterans and adult family members have no military insurance and can’t afford private plans.
Nearly 65,000 rural Alabamians are caught in the coverage gap.
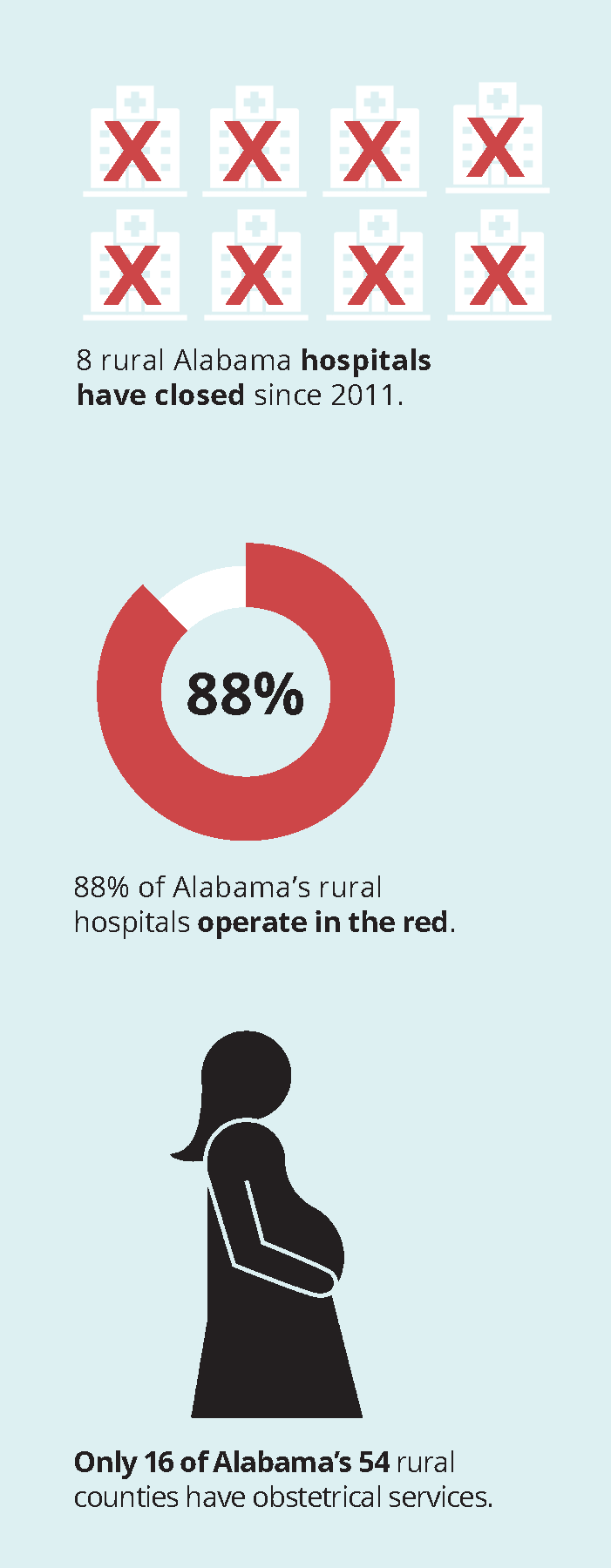
Eight rural Alabama hospitals have closed since 2011.
88% of the state’s rural hospitals operate at a loss.
Alabama’s ‘bare bones’ Medicaid leaves out more than 340,000 people
A family of three with countable income of just $3,841 a year earns too much for the parents to get Medicaid coverage.
As we’ve seen, Alabama Medicaid serves mostly children and people with special health care needs. Only Texas makes it harder for working-age adults without a disability to get Medicaid. First, you have to be a parent of a dependent child. Second, you can’t earn more than 18% of the federal poverty level.
Because of our state’s stringent limits, about 223,000 Alabamians are caught in the coverage gap. Working low-wage jobs that often don’t offer health insurance, they earn too much to qualify for Medicaid and too little to afford private insurance. Some are caught because they’re family caregivers, students, waiting for a disability determination, or working part-time. About 120,000 more are stretching to pay for coverage they can’t afford.
Alabama’s working families need health security
They’re the folks who keep things going — the people who serve our food at restaurants, bag our groceries, patch our roofs and repair our cars. They work hard at economically essential jobs that pay low wages. Yet many of these Alabamians have no affordable health coverage option. As a result, they often struggle to work while dealing with health problems that sap their productivity, add stress to their households and worsen without timely care.
IN FOCUS
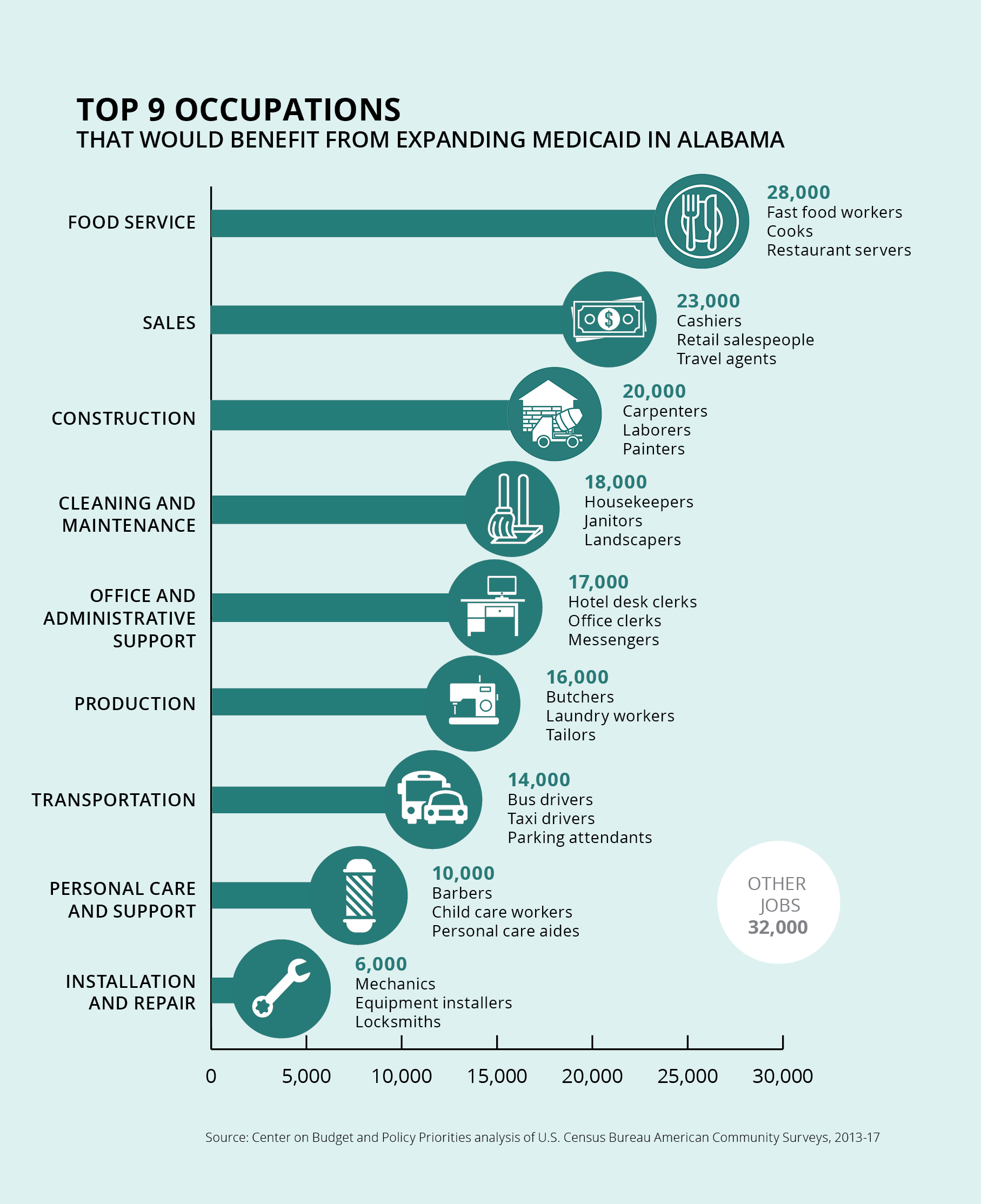
Working Alabamians in the gap
They earn too much to qualify for Medicaid, and they can’t afford employer-based coverage or private insurance. Medicaid expansion would make life better for Alabama’s low-wage workers and strengthen our state’s workforce.
Source: Center on Budget and Policy Priorities analysis of U.S. Census Bureau American Community Surveys, 2013-17
Alabamians who aren’t formally employed need coverage, too
While it’s helpful to highlight the workers in the coverage gap, it’s equally important not to overlook people who don’t hold formal jobs. There are many reasons people in the coverage gap may not be working a regular job. Health coverage is a work support that helps people gain and maintain employment.
SPOTLIGHT
Meet Kenneth Tyrone King
Like thousands of his fellow Alabamians, Kenneth Tyrone King of Birmingham works without health insurance, doing his best to keep chronic health problems under control. (Photo: Julie Bennett)
Kenneth Tyrone King is an “underemployed” resident of Birmingham, where he lives with his wife and daughter. He chooses the term “underemployed” carefully, as a testament to the difficulty of finding and keeping work in the face of chronic health challenges, including an irregular heartbeat. Volunteer work and community advocacy, including service on the Alabama Arise board, give him a sense of connection and purpose, but they don’t pay the bills.
“Most of the jobs I have are temporary,” he says. “And if they do sustain longer-term, they sometimes just end.”
Kenneth isn’t able to obtain health insurance because the work he can get doesn’t provide it. And he can’t afford coverage through the Marketplace.
“I’m thinking about longevity in life and being here for my daughter and my wife,” Kenneth says. “Hopefully, if I can get employment that would have health benefits, that would offset my concerns about my health overall.”
IN FOCUS
Veterans in the health coverage gap
It’s a common misconception that people who serve in the U.S. military automatically receive lifetime eligibility for health coverage and other benefits. In reality, veterans’ health benefits depend on their length of service, military classification, type of discharge and other factors. Treatment for service-connected conditions has no time-of-service requirement, but other health benefits do.
Active-duty service members and their families receive health coverage through the Department of Veterans Affairs (VA). Most also receive “bridge” health insurance coverage in the 180 days before and after their active-duty service. But many Alabama veterans — including many National Guard and Reserve members — return home without military health care for the long term. For the 13,000 Alabama veterans and adult family members who have no military health insurance and can’t afford private plans, the consequences can be dire.
Returning to civilian life can be challenging enough without the added burden of being uninsured. Alabama can show its respect for veterans by giving them the health security they need.
IN FOCUS
Rural Alabamians in the health coverage gap
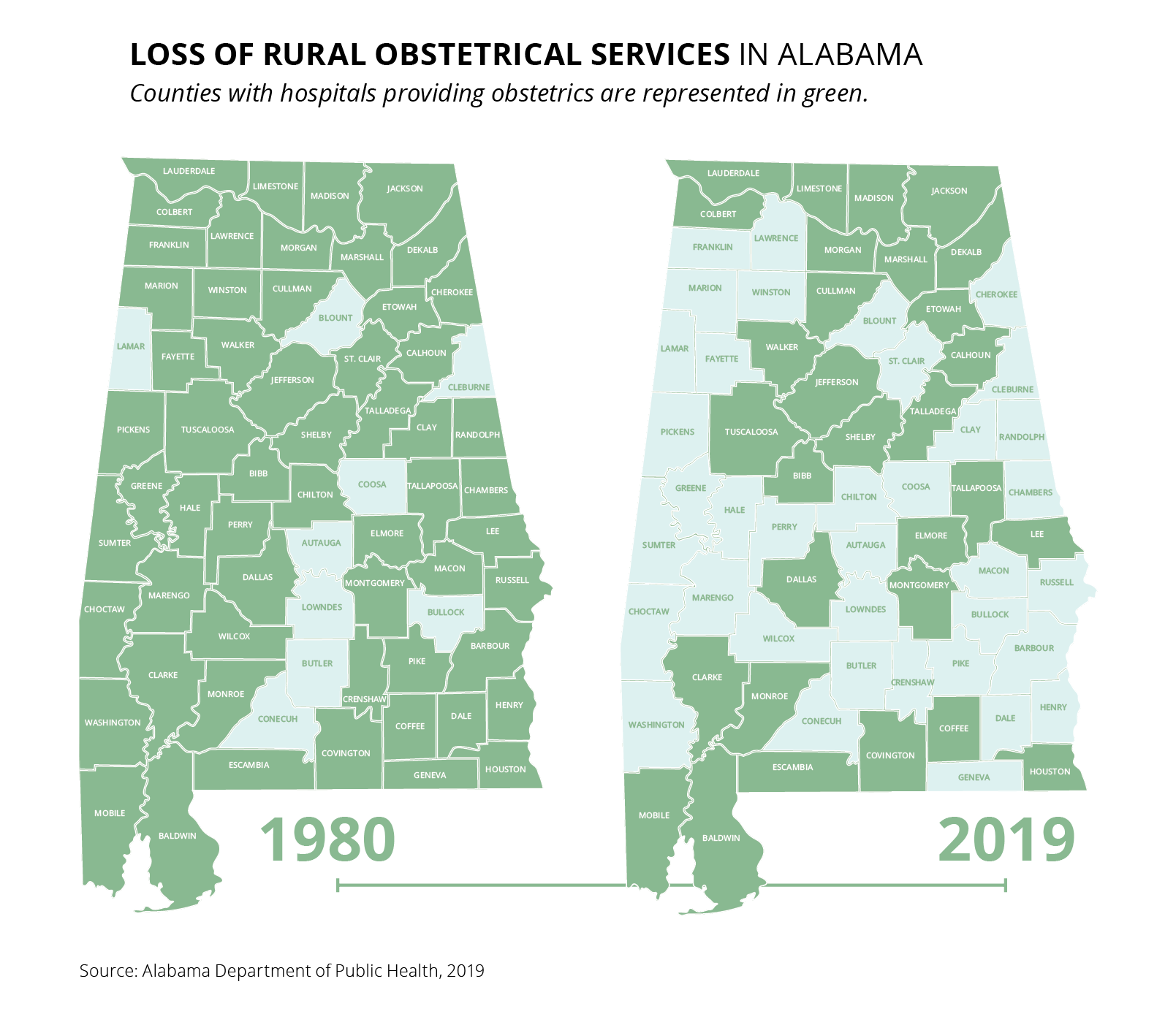
Almost 65,000 rural Alabamians are caught in the health coverage gap, including nearly 4,000 farmers and farm workers. Inadequate health care funding is fraying Alabama’s rural hospital network.
“Rural hospitals in states that increased Medicaid eligibility and enrollment experienced fewer closures,” a 2018 report by the U.S. Government Accountability Office found. Alabama has lost obstetrical services in 29 counties since 1980. Expanding health coverage would protect Alabama’s rural families, hospitals and communities.
Medicaid Matters (Main Section)How does Medicaid work in Alabama? (Section 1)How is Medicaid improving coverage? (Section 2)How can we make Alabama healthier? (Section 4)
Medicaid expansion would help hundreds of thousands of Alabamians get the health care they need.
States that have expanded Medicaid have seen improvements in infant and maternal mortality and greater access to treatment for mental illness and substance use disorders.
Extending coverage would reduce Alabama’s racial health disparities.
Medicaid expansion would generate billions of dollars in economic activity and hundreds of millions of dollars in new tax revenues.
Expanding health coverage would boost efforts to make Alabama’s prison system more humane, restorative and cost-effective.
Medicaid expansion could save hundreds of lives in Alabama every year.
Closing the coverage gap would improve lives
Hundreds of thousands of Alabamians could get the health care they need to survive and thrive if Alabama raised the income limit for Medicaid and allowed coverage for adults who aren’t parents. Medicaid expansion improves lives across a range of health measures, a growing body of research shows. Those areas include better birth outcomes and maternal health, lower overdose rates and improved mental health. Expansion also would increase household financial security and reduce racial health disparities.
Extending coverage would keep Alabamians healthier
Evidence from Medicaid expansion states shows that providing women continuous health coverage before, during and after pregnancy would make a life-saving difference for mothers and babies.
Extending Medicaid coverage to adults with low incomes would extend the benefits of ongoing Medicaid reforms to hundreds of thousands more Alabamians. This improvement would give us the tools we need to address the state’s chronic health challenges, making families and our workforce healthier in the process.
Research shows that Medicaid expansion increases access to treatment for substance use disorders and significantly strengthens responses to the opioid epidemic.
Medicaid expansion would promote racial equity
Alabama’s shameful legacy of segregation and racial discrimination has driven racial health disparities that continue today. Nearly half of uninsured Alabamians with low incomes are people of color, even though people of color make up just one-third of the state’s population. Medicaid expansion would reduce that coverage disparity and increase economic and health security for Alabamians of all racial and ethnic backgrounds.
Medicaid expansion would boost Alabama’s economy and budgets
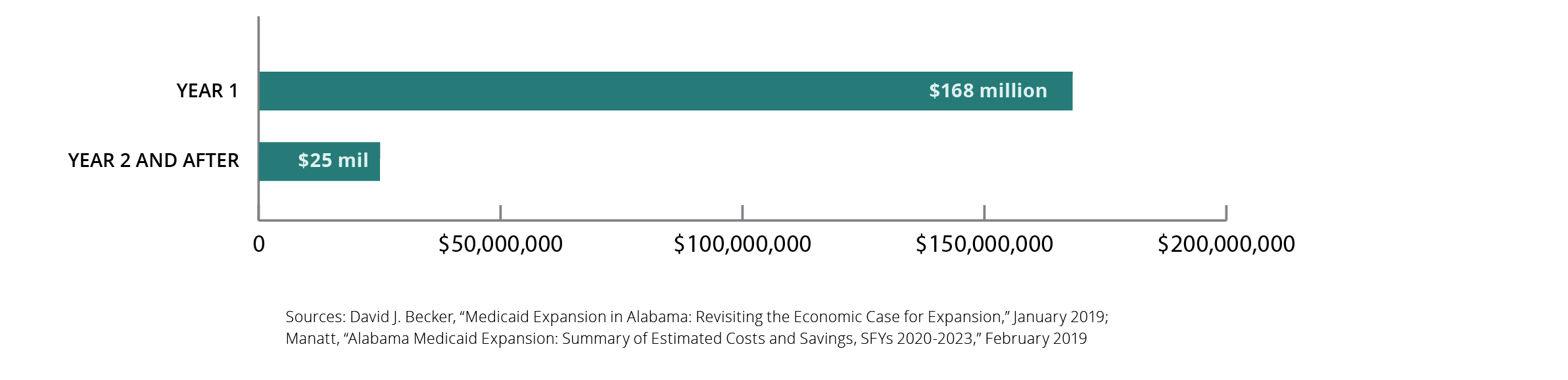
In the first four years of Alabama’s Medicaid expansion, the federal government would spend $6.7 billion for new health coverage in our state. This direct investment would yield:
Covering adults with low incomes also would save $316 million in current state health program costs. With all these gains, the net cost to the state would be:
IN FOCUS
Medicaid expansion would support prison reform in Alabama
In 2019, the U.S. Department of Justice put Alabama on notice that prison violence and overcrowding will trigger federal intervention if we don’t get the problems under control. Medicaid expansion would make our corrections system more humane, restorative and cost-effective in three ways:
Untreated mental illnesses and substance use disorders are major contributors to over-incarceration in Alabama. By strengthening support for these services, Medicaid expansion would reduce recidivism and help more people stay out of the criminal justice system in the first place.
When a person leaves prison, it’s hard to get a job that offers health coverage. But to get and keep a job, you need to be healthy. Medicaid expansion would provide former inmates the health security they need to join and remain in the workforce.
Federal funding would cover 90% of the cost of expansion. That would slash state costs for hospitalizing prisoners and free up funds for other needed investments in the corrections system.
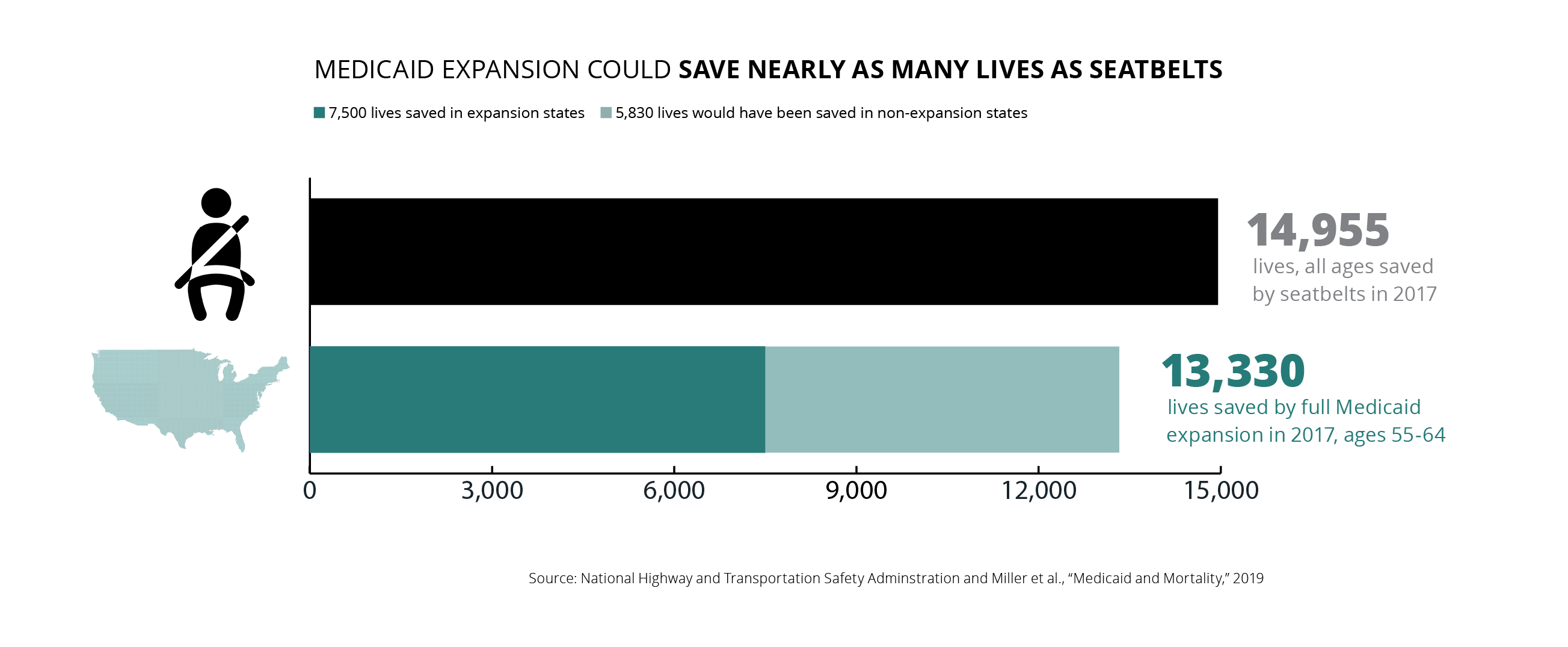
Medicaid expansion’s biggest win: saving lives
Across the country, Medicaid expansion saved the lives of at least 19,200 Americans aged 55 to 64 over the four-year period from 2014 to 2017. During the same period, 768 older Alabamians with low incomes lost their lives because they lacked health insurance. (Source: National Bureau of Economic Research, 2019)
If all states expanded Medicaid, the lives saved each year among older adults would nearly equal those of all ages saved by seatbelts.
SPOTLIGHT
Meet Formeeca Tripp
Formeeca Tripp of Auburn knows firsthand the tough decisions that come with living and working in the coverage gap. (Photo: Julie Bennett)
Formeeca Tripp watched her parents struggle with diabetes and heart disease. She has made efforts to follow a new path. But it hasn’t been easy.
“I have been conditioned to put my health on pause to make sure my children are up to date with all of their health care and mental health needs,” she says.
Formeeca lives in Auburn and is the mother of two children, one of whom was diagnosed with autism. She works full-time as a behavior specialist and part-time as an Uber driver to provide them both with medication they need, sometimes at a great cost to herself. For a long stretch, she fell into the coverage gap. With all her “extra” money spent on her children’s health care needs, Formeeca found herself reporting to work with ailments such as tooth infections and pink eye.
Recently, she gained coverage through her employer’s plan, but many people she knows are not so fortunate. Speaking from her own experience, Formeeca says Alabamians who can’t afford health insurance often work in public-facing jobs.
“It’s the people who are working with the sick and elderly, working with your babies,” she said. “It’s us, out here, hands on, making food, cleaning houses — it’s that gap of people, very important people. People who come into contact with thousands of other people. And you don’t want them to be healthy?”
Medicaid Matters (Main Section)How does Medicaid work in Alabama? (Section 1)How is Medicaid improving coverage? (Section 2)Who’s still left out of health coverage? (Section 3)
Arise’s report, Medicaid Matters: Charting the Course to a Healthier Alabama, illustrates why Medicaid expansion is so critical for the state at this moment in history. Through data, colorful graphics and personal profiles, the report explores Medicaid’s crucial role in Alabama’s health care system. And it reveals how Medicaid expansion would promote racial equity and leave communities better equipped to fight the COVID-19 pandemic.
“Expanding Medicaid would save thousands of lives, create tens of thousands of jobs and help hospitals and clinics across Alabama,” Alabama Arise policy director Jim Carnes said. “As our state continues to struggle with COVID-19, it’s more important than ever for the governor and lawmakers to step up and prove they value the health and well-being of all of our residents.”
Medicaid is a health care lifeline for one in four Alabamians and an economic engine for the entire state. Medicaid Matters explains the Medicaid coverage available to more than 1 million children, seniors, and people with disabilities in Alabama. It highlights improvements that new Medicaid changes are promoting in key areas like infant mortality, obesity and substance use disorders. And it shines a spotlight on more than 340,000 uninsured and underinsured Alabamians who would be covered under Medicaid expansion.
Medicaid expansion would save and transform lives across Alabama
So far, 36 states – including Arkansas, Kentucky and Louisiana – have expanded Medicaid to cover adults with low incomes. But Alabama is one of just 14 states that have not. That remains the case even though the state would get $9 in federal money for every $1 of state funding.
Medicaid expansion would bring peace of mind to thousands of Alabamians who recently lost their jobs and health insurance. And it would make life better for many uninsured people who are working on the front lines of the pandemic. This includes workers at grocery stores, hospitals, child care facilities and other essential businesses.
Formeeca Tripp, a behavior specialist who lives in Auburn, explains in Arise’s report how the health of any Alabamian is linked to the health of every Alabamian.
Formeeca Tripp of Auburn knows firsthand the tough decisions that come with living and working in the coverage gap. (Photo: Julie Bennett)
“It’s the people who are working with the sick and elderly, working with your babies,” Tripp said. “It’s us, out here, hands on, making food, cleaning houses – it’s that gap of people, very important people. People who come into contact with thousands of other people. And you don’t want them to be healthy?”
Arise’s statewide online summer listening sessions are a chance to hear what’s happening on key state policy issues and share your vision for our 2021 policy agenda. Register now to help identify emerging issues and inform our work to build a better Alabama.
We’d love to see you at any or all of these sessions! Registration is required, so please register at the link under each description.
June 23rd, 6 p.m. –Money talks
How can we strengthen education, health care, child care and other services that help Alabamians make ends meet? And how can we fund those services more equitably? Click here to register for this session.









 Medicaid pumps $7 billion in federal and state money into our health care system every year. Without Medicaid funding, many of the doctors’ offices, clinics, hospitals and other medical facilities that all Alabamians depend on would have to cut services or close.
Medicaid pumps $7 billion in federal and state money into our health care system every year. Without Medicaid funding, many of the doctors’ offices, clinics, hospitals and other medical facilities that all Alabamians depend on would have to cut services or close.